Ada Form Pdf
Ada Form Pdf - Policyholder/subscriber id (assigned by plan) patient information 18. Relationship to policyholder/subscriber in #12 above self spouse dependent child other 19. The purpose of this form is to assist the university in determining whether, or to what extent, a reasonable accommodation is required Name of policyholder/subscriber in #4 (last, first, middle initial, sufix) 6. Title ii state and local government facilities must follow the requirements of the 2010 standards, Americans with disabilities act (ada) accommodation request form. Form completion instructions are provided for each data item, which is indicated by a number. Reserved for future use f u 9. Web follow link ada 2019 claim form completion instructions.pdf ada 2019 dental claim form_j430.pdf 1 Web the americans with disabilities act (ada) protects people with disabilities from discrimination.
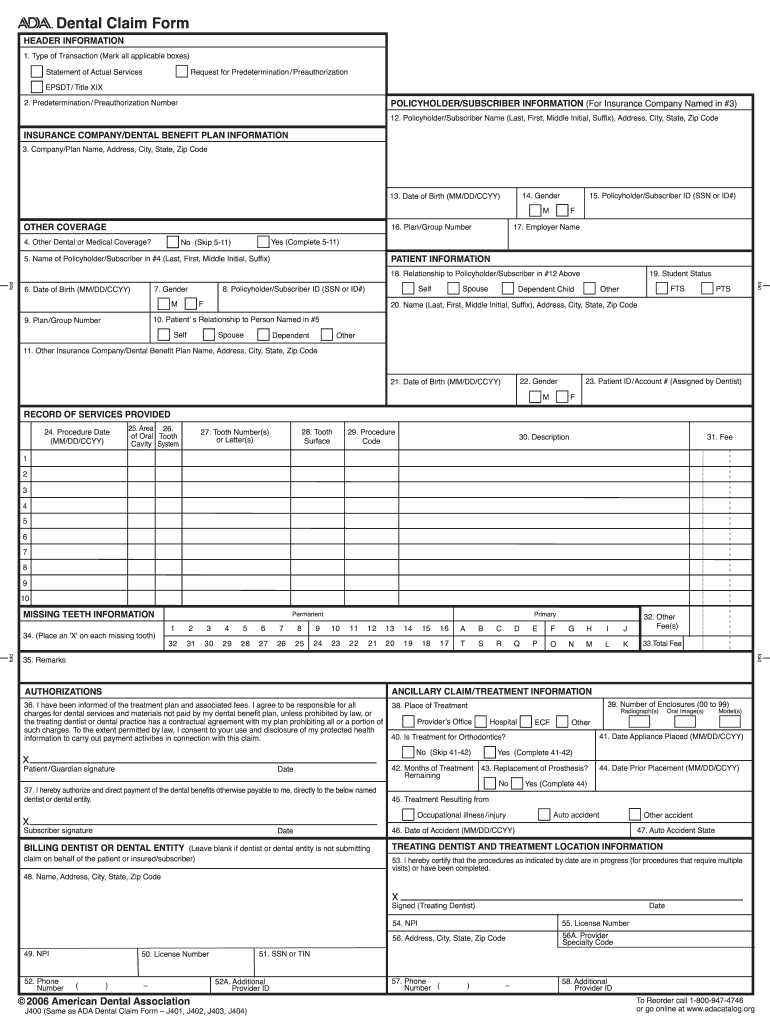
Americans with disabilities act (ada) accommodation request form. Name of policyholder/subscriber in #4 (last, first, middle initial, sufix) 6. The following materials are prepared by ada practice institute staff with contributions from the ada council. Web the ada dental claim form provides a common format for reporting dental services to a patient's dental benefit plan. Version 2024 © american dental association. 2010 standards for state and local government facilities: The purpose of this form is to assist the university in determining whether, or to what extent, a reasonable accommodation is required Web the americans with disabilities act (ada) protects people with disabilities from discrimination. Date of birth (mm/dd/ccyy) 7. Title ii state and local government facilities must follow the requirements of the 2010 standards,
Policyholder/subscriber id (assigned by plan) patient information 18. Americans with disabilities act (ada) accommodation request form. Web the ada dental claim form provides a common format for reporting dental services to a patient's dental benefit plan. The following materials are prepared by ada practice institute staff with contributions from the ada council. Date of birth (mm/dd/ccyy) 7. From voting to parking, the ada is a law that protects people with disabilities in many areas of public life. Version 2024 © american dental association. Web the americans with disabilities act (ada) protects people with disabilities from discrimination. Physical or mental impairment (as opposed to the medical need of a family member)? Complete this section for all requests.
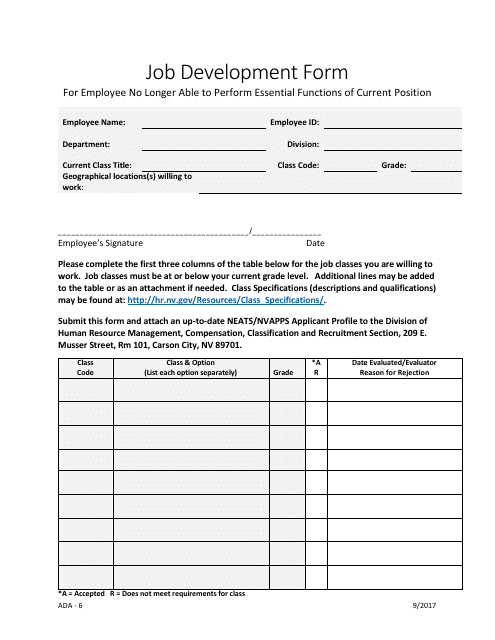
Form ADA6 Download Fillable PDF or Fill Online Job Development Form
2010 standards for state and local government facilities: Any updates to these instructions will be posted on the ada’s web site (ada.org). Name of policyholder/subscriber in #4 (last, first, middle initial, sufix) 6. Web the ada dental claim form provides a common format for reporting dental services to a patient's dental benefit plan. Reserved for future use f u 9.
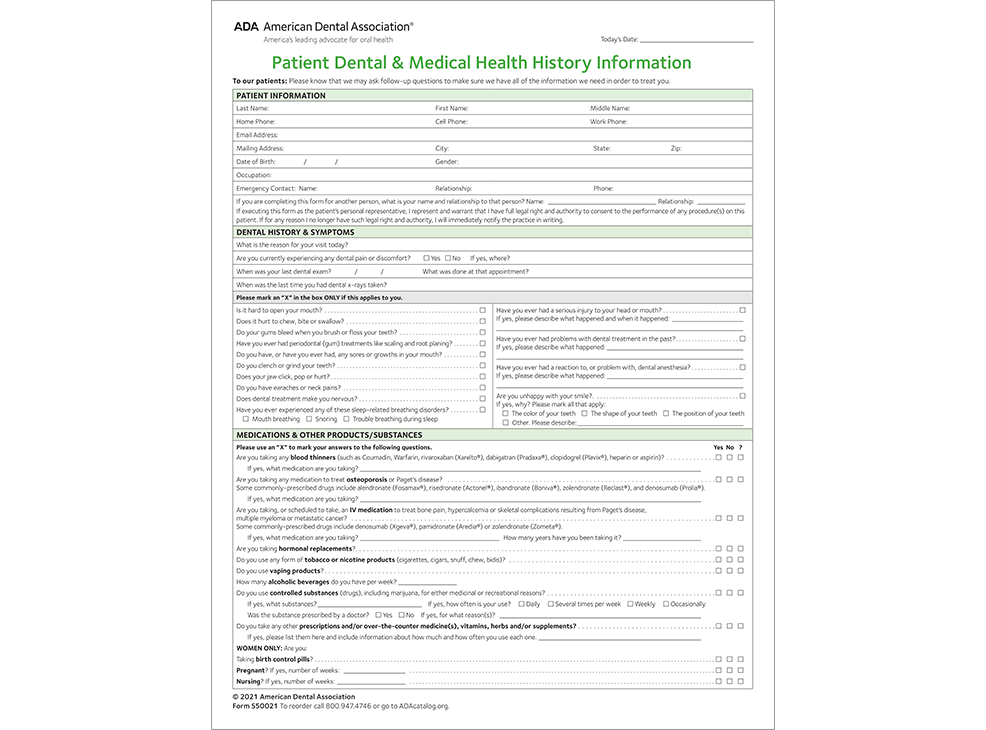
ADA Patient Health History Form S50021
Web comprehensive ada dental claim form completion instructions are printed in the cdt manual. Ada policy promotes use and acceptance of the most current version of the ada dental claim form by dentists and payers. Web ada job accommodation request and medical inquiry form. Name of policyholder/subscriber in #4 (last, first, middle initial, sufix) 6. 2010 standards for state and.
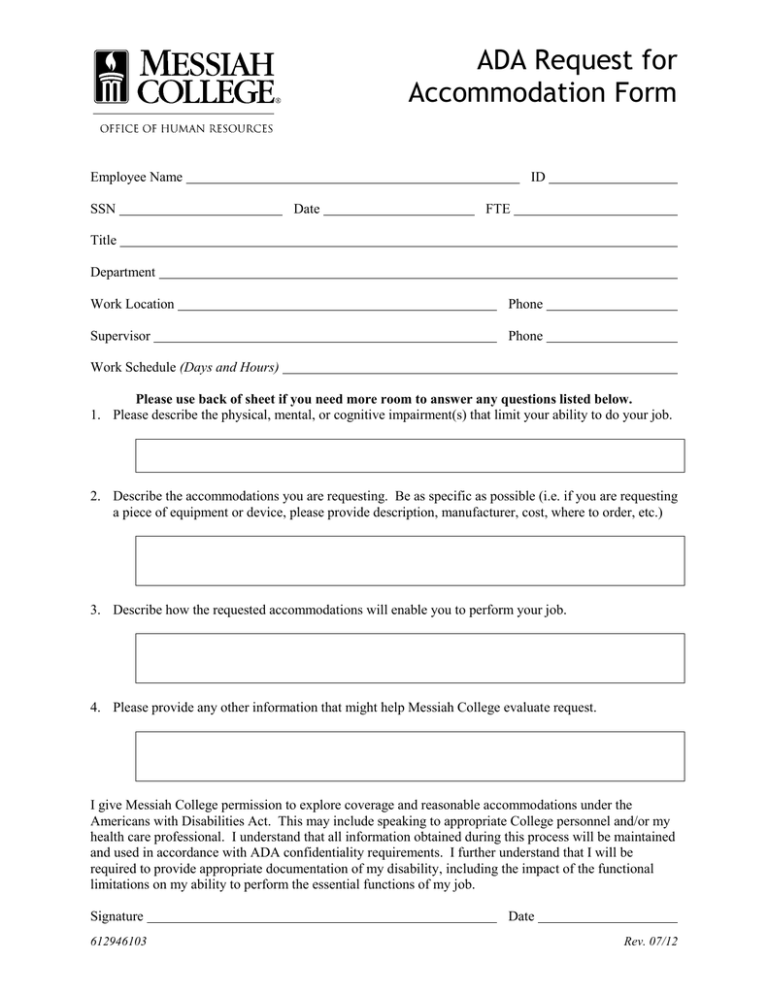
ADA Request for Form
Policyholder/subscriber id (assigned by plan) patient information 18. Title ii state and local government facilities must follow the requirements of the 2010 standards, The purpose of this form is to assist the university in determining whether, or to what extent, a reasonable accommodation is required 2010 standards for state and local government facilities: Web comprehensive ada dental claim form completion.

Ada Health History Form 20202022 Fill and Sign Printable Template
American’s with disabilities act (ada) and american’s with disabilities act amendments act (adaaa). Americans with disabilities act (ada) accommodation request form. Reserved for future use f u 9. Web ada dental claim form completion instructions. Policyholder/subscriber id (assigned by plan) patient information 18.
Printable Ada Claim Form 2021 Printable World Holiday
Web ada dental claim form completion instructions. Disability rights are civil rights. Form completion instructions are provided for each data item, which is indicated by a number. From voting to parking, the ada is a law that protects people with disabilities in many areas of public life. Are you requesting accommodation because of your.
Form 133.3 Download Fillable PDF or Fill Online Ada
Complete this section for all requests. The purpose of this form is to assist the university in determining whether, or to what extent, a reasonable accommodation is required Date of birth (mm/dd/ccyy) 7. Title ii state and local government facilities must follow the requirements of the 2010 standards, Web ada job accommodation request and medical inquiry form.

ADA full form YouTube
The following materials are prepared by ada practice institute staff with contributions from the ada council. Web ada job accommodation request and medical inquiry form. Web follow link ada 2019 claim form completion instructions.pdf ada 2019 dental claim form_j430.pdf 1 Web comprehensive ada dental claim form completion instructions are printed in the cdt manual. From voting to parking, the ada.

Fill Free fillable ADA COVID19 Daily Screening Log 200511 RE PDF form
The purpose of this form is to assist the university in determining whether, or to what extent, a reasonable accommodation is required Web the americans with disabilities act (ada) protects people with disabilities from discrimination. Physical or mental impairment (as opposed to the medical need of a family member)? Version 2024 © american dental association. Ada policy promotes use and.
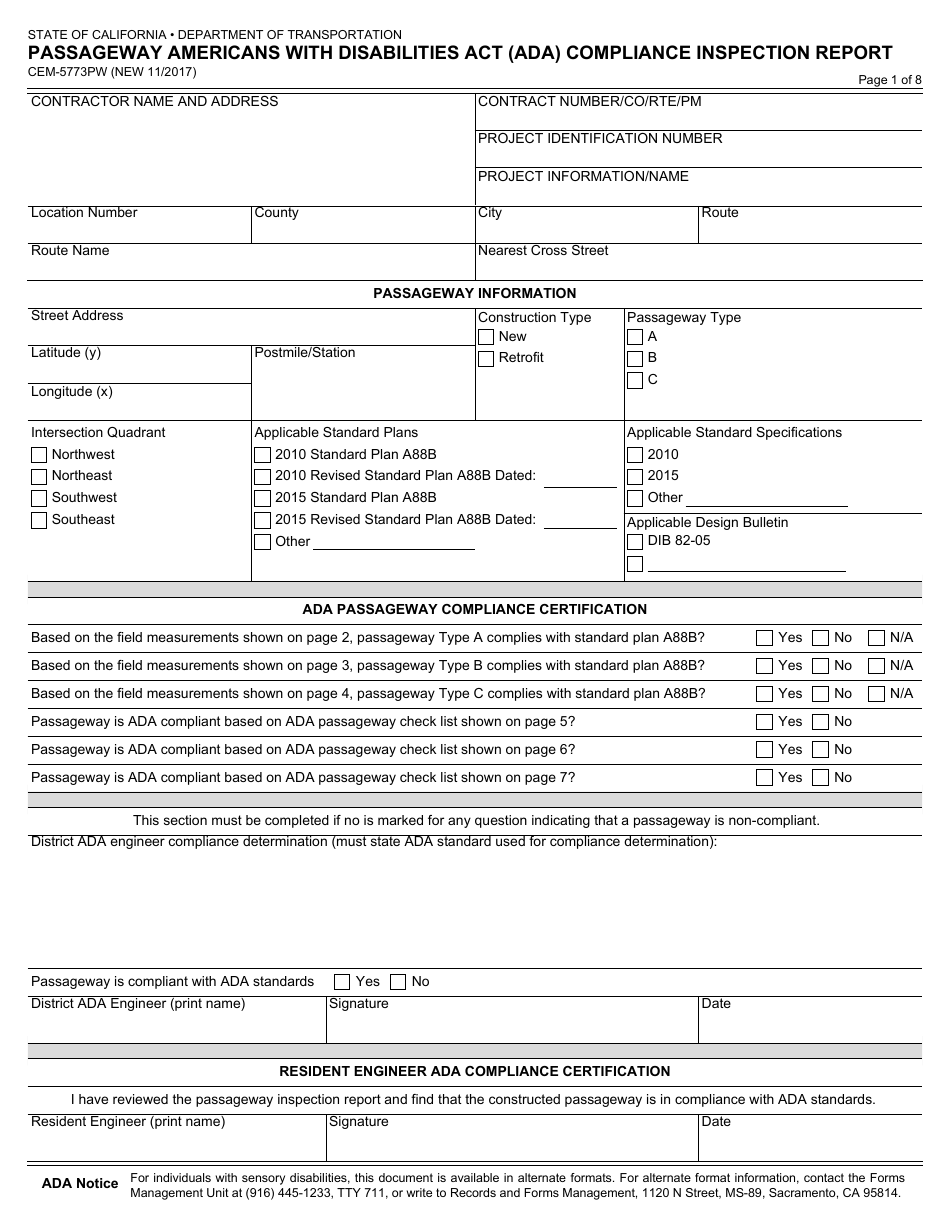
Form CEM5773PW Download Fillable PDF or Fill Online Passageway
Reserved for future use f u 9. Complete this section for all requests. Ada policy promotes use and acceptance of the most current version of the ada dental claim form by dentists and payers. Are you requesting accommodation because of your. The purpose of this form is to assist the university in determining whether, or to what extent, a reasonable.

Form BDE3101 Download Fillable PDF or Fill Online Ada Statement of
Ada policy promotes use and acceptance of the most current version of the ada dental claim form by dentists and payers. The purpose of this form is to assist the university in determining whether, or to what extent, a reasonable accommodation is required Are you requesting accommodation because of your. Note that data items are in. Form completion instructions are.
Date Of Birth (Mm/Dd/Ccyy) 7.
Note that data items are in. Complete this section for all requests. Ada policy promotes use and acceptance of the most current version of the ada dental claim form by dentists and payers. Title ii state and local government facilities must follow the requirements of the 2010 standards,
Web The Ada Dental Claim Form Provides A Common Format For Reporting Dental Services To A Patient's Dental Benefit Plan.
Web ada dental claim form completion instructions. Any updates to these instructions will be posted on the ada’s web site (ada.org). Web follow link ada 2019 claim form completion instructions.pdf ada 2019 dental claim form_j430.pdf 1 Web ada job accommodation request and medical inquiry form.
Version 2024 © American Dental Association.
Physical or mental impairment (as opposed to the medical need of a family member)? The following materials are prepared by ada practice institute staff with contributions from the ada council. Web comprehensive ada dental claim form completion instructions are printed in the cdt manual. The purpose of this form is to assist the university in determining whether, or to what extent, a reasonable accommodation is required
Relationship To Policyholder/Subscriber In #12 Above Self Spouse Dependent Child Other 19.
Policyholder/subscriber id (assigned by plan) patient information 18. Are you requesting accommodation because of your. Disability rights are civil rights. Web the americans with disabilities act (ada) protects people with disabilities from discrimination.