Blue Cross Blue Shield Health Benefits Claim Form
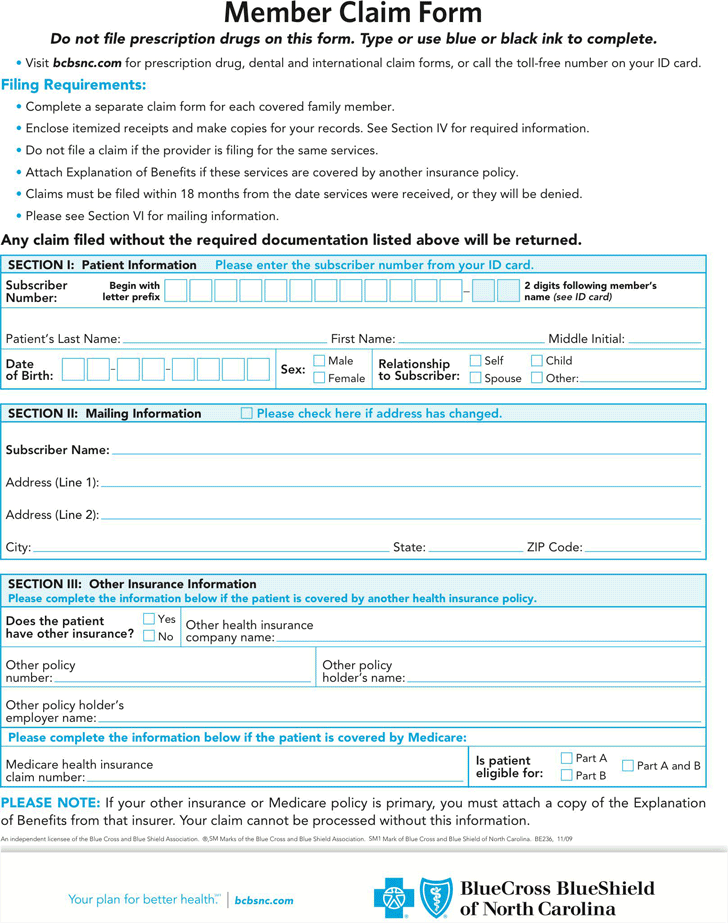
Blue Cross Blue Shield Health Benefits Claim Form - Web health benefits claim form. Claims for all other services should be sent to your local blue cross/blue shield plan using a federal employee program health benefits claim form. Web before submitting your claim, please be sure that: Patient information please enter the subscriber number from your id card. Create professional documents with signnow. Begin with letter prefix 2 digits following member’s name (see id card) patient’s last name: Web health benefits claim form please complete a separate claim form for each family member. Web forms and documents for individuals and families. Please have your id prefix ready to enter before searching for your plan form. Medical or vision claim form.
Forms for blue care network (hmo) members. Male female relationship to subscriber: Horizon hmo, horizon pos, horizon direct access, horizon epo, horizon ppo, traditional, national accounts and omnia health plan members use this form for medical claims. Access all the forms and documents you need to manage your health plan—from claims forms to health information disclosures. Search by keywords, or filter by category or year, to. Web to have a claim form mailed to you, call member services at the phone number on the back of your member id card. Web if you're a blue cross blue shield of michigan member, use this form to ask for reimbursement for medical, hearing and vision services you've had to pay for yourself. Need to submit a claim? (for example, if your service was provided on march 5, 2022, you have until december 31, 2023 to submit your claim). You can use our interactive search to find your local blue cross blue shield company's website.
Replace your member id card. Blue cross and blue shield companies across the country can help. You have kept copies of each document and bill for your personal records the claim form and all related materials should be submitted to: Example of claims sent to your local blue cross and/or blue shield plan includes: Medical/dental claims pharmacy claims blue cross and blue shield global core international claims log in to fast forms create account & log. Begin with letter prefix 2 digits following member’s name (see id card) patient’s last name: Male female relationship to subscriber: Claims for all other services should be sent to your local blue cross/blue shield plan using a federal employee program health benefits claim form. Web horizon health insurance claim form. Only claims for prescriptions purchased from a retail pharmacy are to be sent to the address on the front.
Free Blue Cross Blue Shield Association Member Claim Form PDF 90KB
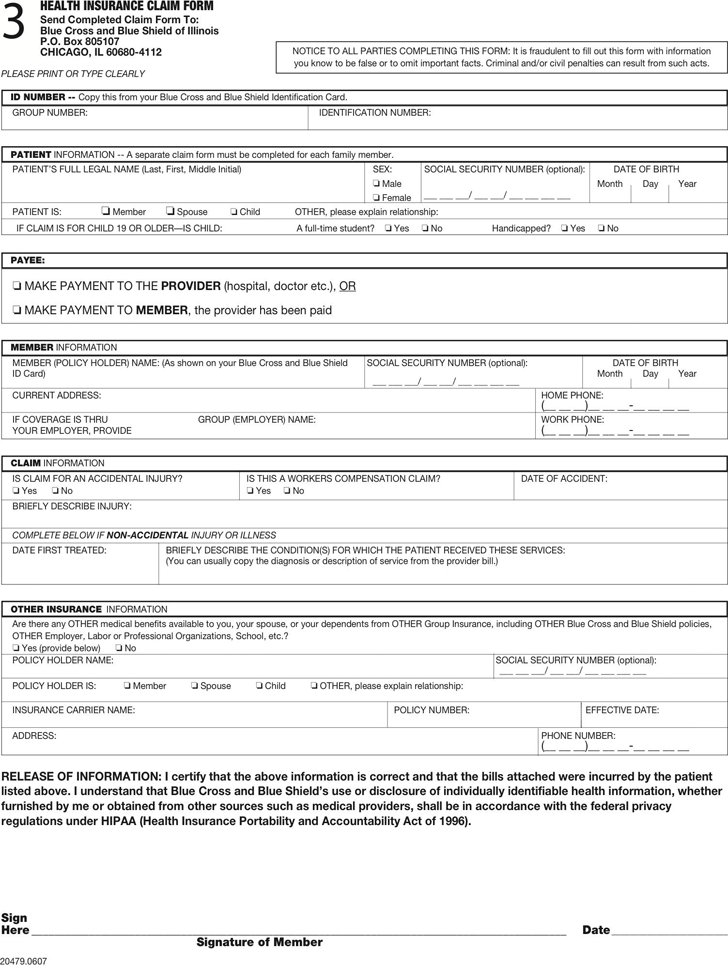
Web r patient’s name (first, middle initial and last) health benefits claim form identification number patient’s dat e of birth month/day/year patient’s sex male female name of enrollee or policy holder (first, middle initial and last) date of birth month/day/year patient’s relationship to. Example of claims sent to your local blue cross and/or blue shield plan includes: Is the business.
Blue Cross Blue Shield Appeal Form / Fitness Benefit Form Blue Cross
Web horizon health insurance claim form. Is the business name of group hospitalization and medical services, inc. Prescription drug claim forms (ppo and hmo) Overseas members should use the overseas medical claim form. Only claims for prescriptions purchased from a retail pharmacy are to be sent to the address on the front.
Free Blue Cross Blue Shield Association Medical Claim Form PDF
Overseas members should use the overseas medical claim form. Web claim form to pay insured/subscriber each item on this form needs to be completed. Web health benefits claim form. Download and complete the appropriate form below, then submit it by december 31 of the year following the year that you received service. If you use a provider outside of the.
Guide to Blue Cross Blue Shield Coverage for Addiction Treatment Centers
Begin with letter prefix 2 digits following member’s name (see id card) patient’s last name: Web how to submit a claim. Search by keywords, or filter by category or year, to. Your local company can help you to: Web claim form to pay insured/subscriber each item on this form needs to be completed.

Free Printable Medical Claim Forms
The itemized bills are attached. Web before submitting your claim, please be sure that: File or check on claim. Web claim form to pay insured/subscriber each item on this form needs to be completed. (for example, if your service was provided on march 5, 2022, you have until december 31, 2023 to submit your claim).
Empire Blue Cross Blue Shield Claim Form Fill Out and Sign Printable
Web how to submit a claim. Get your fillable template and complete it online using the instructions provided. You can also submit your claim online or through the blue cross blue shield global core mobile app. File or check on claim. Web to have a claim form mailed to you, call member services at the phone number on the back.

How are Blue Cross and Blue Shield health insurers controlled and
Estimate the cost of a medical procedure. Is the business name of group hospitalization and medical services, inc. You have kept copies of each document and bill for your personal records the claim form and all related materials should be submitted to: Overseas members should use the overseas medical claim form. Medical or vision claim form.

blue cross blue shield health insurance claim form Google Search
Claims for all other services should be sent to your local blue cross/blue shield plan using a federal employee program health benefits claim form. Access all the forms and documents you need to manage your health plan—from claims forms to health information disclosures. Is the business name of group hospitalization and medical services, inc. Web claim form to pay insured/subscriber.

Blue Cross Blue Shield Overseas Claim Form Fill Online, Printable
Do not use to submit prescription drug services. (for example, if your service was provided on march 5, 2022, you have until december 31, 2023 to submit your claim). Web blue cross blue shield global core forms. Horizon hmo, horizon pos, horizon direct access, horizon epo, horizon ppo, traditional, national accounts and omnia health plan members use this form for.
2008 Form AL BCBS MKT148 Fill Online, Printable, Fillable, Blank
Web blue cross blue shield global core forms. Web forms and documents for individuals and families. Overseas members should use the overseas medical claim form. Also use for vision services including eyewear. Web if you're a blue cross blue shield of michigan member, use this form to ask for reimbursement for medical, hearing and vision services you've had to pay.
The Claim Form Is Fully Completed And Signed.
Horizon hmo, horizon pos, horizon direct access, horizon epo, horizon ppo, traditional, national accounts and omnia health plan members use this form for medical claims. Forms for blue cross blue shield of michigan (ppo) members. Replace your member id card. Male female relationship to subscriber:
(For Example, If Your Service Was Provided On March 5, 2022, You Have Until December 31, 2023 To Submit Your Claim).
The mailing address for your local plan can be located on fepblue.org by using the following link: Prescription drug claim forms (ppo and hmo) Access all the forms and documents you need to manage your health plan—from claims forms to health information disclosures. Web member claim form section 1:
Web R Patient’s Name (First, Middle Initial And Last) Health Benefits Claim Form Identification Number Patient’s Dat E Of Birth Month/Day/Year Patient’s Sex Male Female Name Of Enrollee Or Policy Holder (First, Middle Initial And Last) Date Of Birth Month/Day/Year Patient’s Relationship To.
Patient information please enter the subscriber number from your id card. If you use a provider outside of the network, you will need to complete and file a claim form for reimbursement. Claims for all other services should be sent to your local blue cross/blue shield plan using a federal employee program health benefits claim form. Create professional documents with signnow.
Web Complete A Blue Cross Blue Shield Global Core International Claim Form And Send It With The Bill(S) To The Service Center (The Address Is On The Form).
Web blue cross blue shield global core forms. The itemized bills are attached. Need to submit a claim? Web health benefits claim form.