Caremark Prior Auth Form
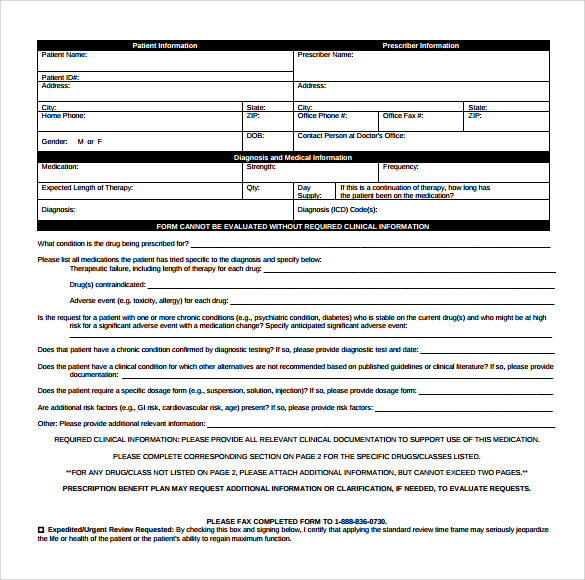
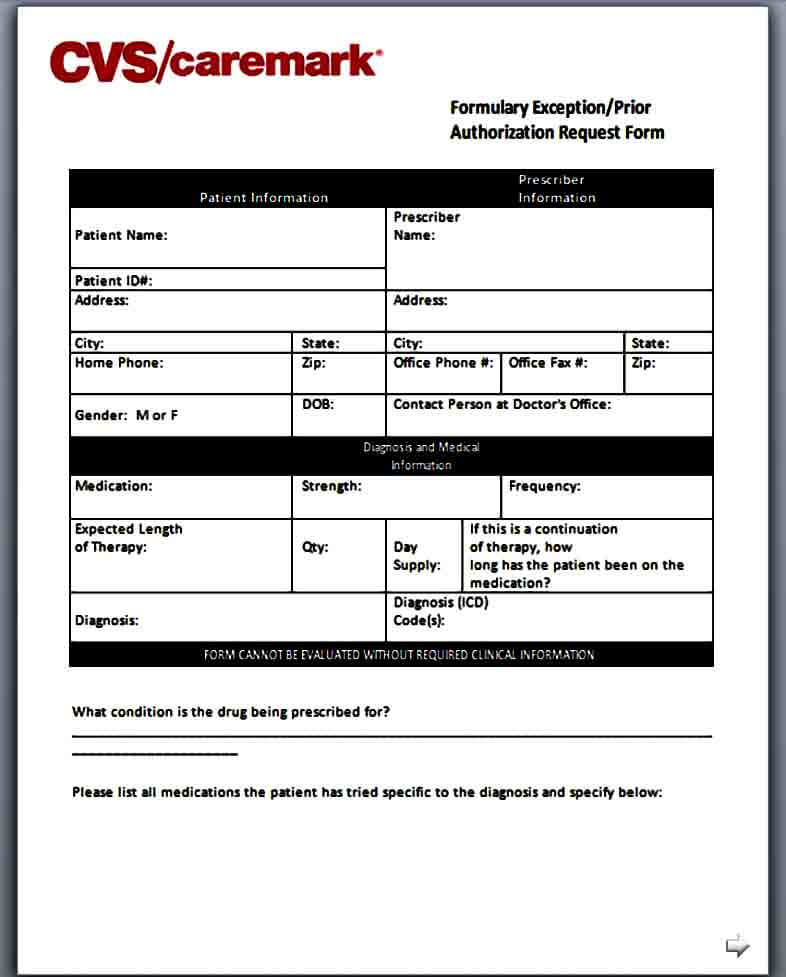
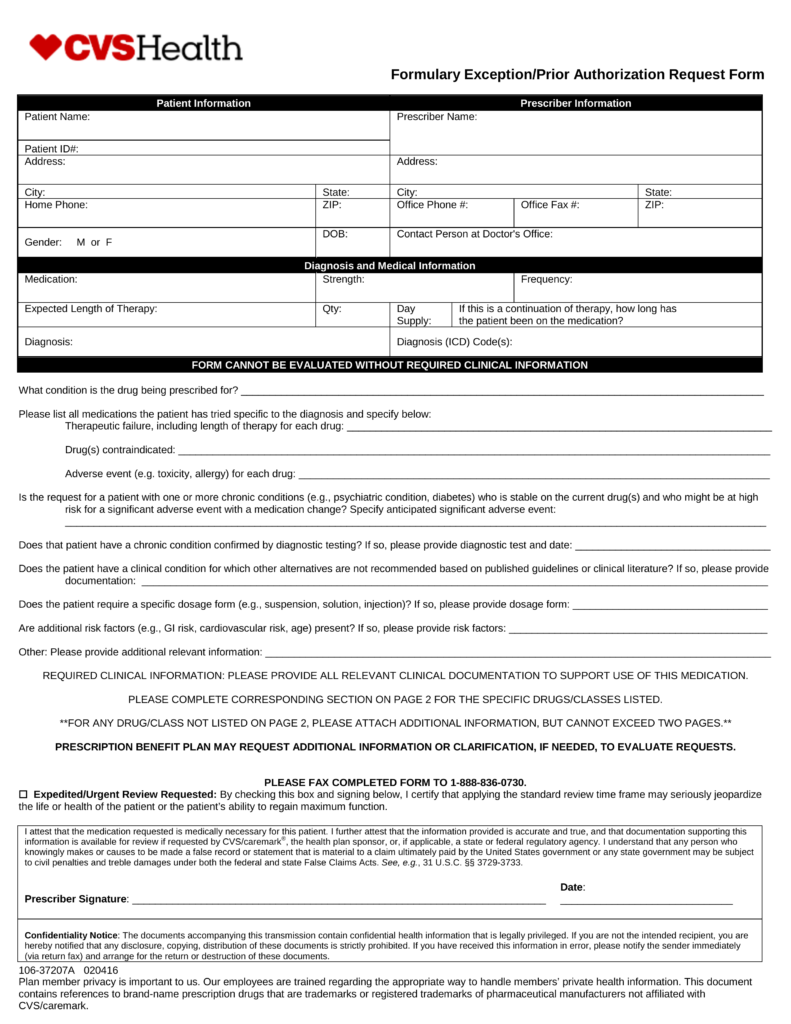
Caremark Prior Auth Form - Web formulary exception/prior authorization request form patient information prescriber information patient name: Cvs caremark prior authorization (pa) tools are developed to ensure safe, effective and appropriate use of selected drugs. Please complete corresponding section for these specific drugs/classes listed below and circle the appropriate. Web this is called prior authorization, or pa, and it means that your doctor will have to provide additional information on why they are prescribing this medication for you. Covermymeds is cvs caremark prior authorization forms’s preferred method for receiving epa requests. Web download, review and print the prior approval form for the requested medication. Select the starting letter of the name of the medication to begin. Once we receive your request, we will fax you a drug specific prior authorization request form along with the patient’s specific information and questions that must be answered. A physician will need to fill in the form with the patient’s medical information and submit it to cvs/caremark for assessment. A abilify mycite absorica (brand only) abstral aciphex (generic only) actemra acthar gel actimmune actiq aczone adakveo adbry
By checking this box and signing below, i certify that applying the standard review time frame may seriously jeopardize the life or health of the patient or the patient’s ability to regain maximum function. Covermymeds automates the prior authorization (pa) process making it the fastest and easiest way to review, complete and track pa requests. We've partnered with covermymeds ® and surescripts ®, making it easy for you to access electronic prior authorization (epa) via the epa vendor of your choice. Web prior authorization forms pa forms for physicians when a pa is needed for a prescription, the member will be asked to have the physician or authorized agent of the physician contact our prior authorization department to answer criteria questions to determine coverage. Use the arrows next to each medication name to expand your selection. Web formulary exception/prior authorization request form expedited/urgent review requested: A physician will need to fill in the form with the patient’s medical information and submit it to cvs/caremark for assessment. Web updated june 02, 2022. Covermymeds is cvs caremark prior authorization forms’s preferred method for receiving epa requests. Select the starting letter of the name of the medication to begin.
Select the starting letter of the name of the medication to begin. Some automated decisions may be communicated in less than 6 seconds! Web this is called prior authorization, or pa, and it means that your doctor will have to provide additional information on why they are prescribing this medication for you. A abilify mycite absorica (brand only) abstral aciphex (generic only) actemra acthar gel actimmune actiq aczone adakveo adbry Web formulary exception/prior authorization request form expedited/urgent review requested: Web download, review and print the prior approval form for the requested medication. Web select the appropriate cvs caremark form to get started. Web formulary exception/prior authorization request form patient information prescriber information patient name: Cvs caremark reviews this information and, based on your plan, determines whether or not the medication will be covered. Web cvs caremark has made submitting pas easier and more convenient.
FREE 8+ Sample Caremark Prior Authorization Forms in PDF
Some automated decisions may be communicated in less than 6 seconds! Covermymeds automates the prior authorization (pa) process making it the fastest and easiest way to review, complete and track pa requests. Web formulary exception/prior authorization request form patient information prescriber information patient name: Please complete corresponding section for these specific drugs/classes listed below and circle the appropriate. A physician.
Template Caremark Prior Authorization Form Mous Syusa
A cvs/caremark prior authorization form is to be used by a medical office when requesting coverage for a cvs/caremark plan member’s prescription. Web select the appropriate cvs caremark form to get started. Some automated decisions may be communicated in less than 6 seconds! Once we receive your request, we will fax you a drug specific prior authorization request form along.

cvscaremarkpriorauthorizationform600x800 Free Job Application Form
Web prior authorization forms pa forms for physicians when a pa is needed for a prescription, the member will be asked to have the physician or authorized agent of the physician contact our prior authorization department to answer criteria questions to determine coverage. By checking this box and signing below, i certify that applying the standard review time frame may.

Cvs Caremark Appeal Form Fill Out and Sign Printable PDF Template
Web cvs caremark has made submitting pas easier and more convenient. A physician will need to fill in the form with the patient’s medical information and submit it to cvs/caremark for assessment. Covermymeds automates the prior authorization (pa) process making it the fastest and easiest way to review, complete and track pa requests. By checking this box and signing below,.
Free CVS/Caremark Prior (Rx) Authorization Form PDF eForms
By checking this box and signing below, i certify that applying the standard review time frame may seriously jeopardize the life or health of the patient or the patient’s ability to regain maximum function. Web prior authorization forms pa forms for physicians when a pa is needed for a prescription, the member will be asked to have the physician or.

Cvs Caremark Prior Auth Form Pdf
Please complete corresponding section for these specific drugs/classes listed below and circle the appropriate. Web formulary exception/prior authorization request form expedited/urgent review requested: Covermymeds is cvs caremark prior authorization forms’s preferred method for receiving epa requests. We've partnered with covermymeds ® and surescripts ®, making it easy for you to access electronic prior authorization (epa) via the epa vendor of.
FREE 8+ Sample Prior Authorization Forms in PDF MS Word
Please complete corresponding section for these specific drugs/classes listed below and circle the appropriate. We've partnered with covermymeds ® and surescripts ®, making it easy for you to access electronic prior authorization (epa) via the epa vendor of your choice. Cvs caremark reviews this information and, based on your plan, determines whether or not the medication will be covered. Web.

Template Caremark Prior Authorization Form Mous Syusa
Web prior authorization forms pa forms for physicians when a pa is needed for a prescription, the member will be asked to have the physician or authorized agent of the physician contact our prior authorization department to answer criteria questions to determine coverage. Select the starting letter of the name of the medication to begin. Some automated decisions may be.

CVS Caremark 10637207A 20192021 Fill and Sign Printable Template
Web updated june 02, 2022. Cvs caremark reviews this information and, based on your plan, determines whether or not the medication will be covered. We've partnered with covermymeds ® and surescripts ®, making it easy for you to access electronic prior authorization (epa) via the epa vendor of your choice. Web select the appropriate cvs caremark form to get started..

Info Caremark Epa Form Fill Out and Sign Printable PDF Template signNow
Web updated june 02, 2022. By checking this box and signing below, i certify that applying the standard review time frame may seriously jeopardize the life or health of the patient or the patient’s ability to regain maximum function. Once we receive your request, we will fax you a drug specific prior authorization request form along with the patient’s specific.
Covermymeds Is Cvs Caremark Prior Authorization Forms’s Preferred Method For Receiving Epa Requests.
Web formulary exception/prior authorization request form expedited/urgent review requested: Web updated june 02, 2022. Some automated decisions may be communicated in less than 6 seconds! Web download, review and print the prior approval form for the requested medication.
We've Partnered With Covermymeds ® And Surescripts ®, Making It Easy For You To Access Electronic Prior Authorization (Epa) Via The Epa Vendor Of Your Choice.
Use the arrows next to each medication name to expand your selection. Cvs caremark reviews this information and, based on your plan, determines whether or not the medication will be covered. Web prior authorization forms pa forms for physicians when a pa is needed for a prescription, the member will be asked to have the physician or authorized agent of the physician contact our prior authorization department to answer criteria questions to determine coverage. Web select the appropriate cvs caremark form to get started.
Select The Starting Letter Of The Name Of The Medication To Begin.
Cvs caremark prior authorization (pa) tools are developed to ensure safe, effective and appropriate use of selected drugs. Web cvs caremark has made submitting pas easier and more convenient. A physician will need to fill in the form with the patient’s medical information and submit it to cvs/caremark for assessment. Covermymeds automates the prior authorization (pa) process making it the fastest and easiest way to review, complete and track pa requests.
By Checking This Box And Signing Below, I Certify That Applying The Standard Review Time Frame May Seriously Jeopardize The Life Or Health Of The Patient Or The Patient’s Ability To Regain Maximum Function.
Once we receive your request, we will fax you a drug specific prior authorization request form along with the patient’s specific information and questions that must be answered. A abilify mycite absorica (brand only) abstral aciphex (generic only) actemra acthar gel actimmune actiq aczone adakveo adbry A cvs/caremark prior authorization form is to be used by a medical office when requesting coverage for a cvs/caremark plan member’s prescription. Web formulary exception/prior authorization request form patient information prescriber information patient name: