Cms 1500 Form Completed Example
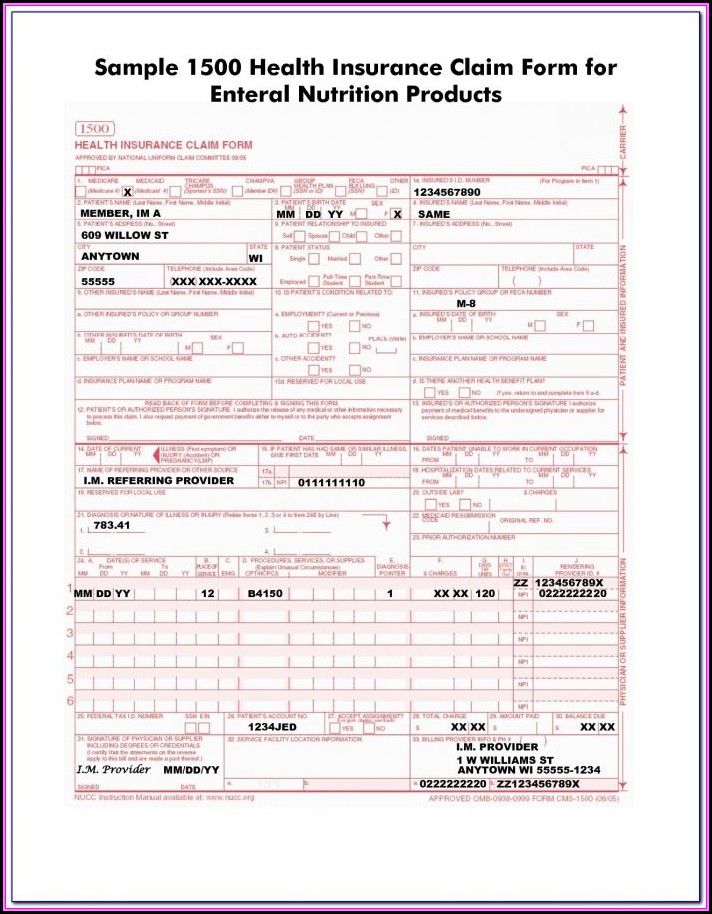
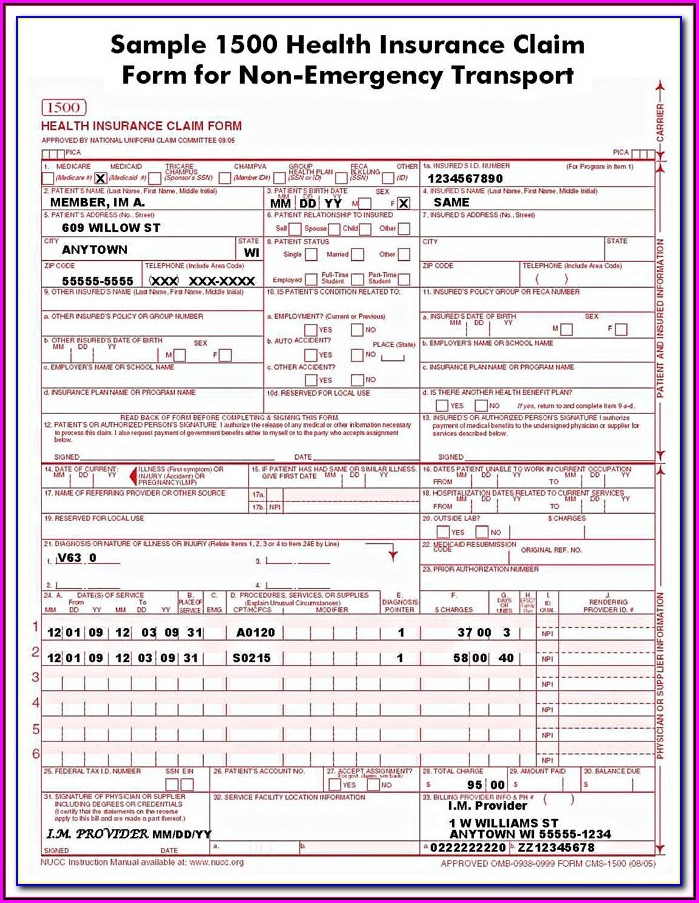
Cms 1500 Form Completed Example - Insured’s address (no., street) city state zip code telephone (include area code) 11. The form is used by physicians and allied health professionals to submit claims for medical services. Sign up to get the latest information about your choice of cms topics. Write down the patient's full name, birth date, sex, and address. Refer to the nucc website for further detailed instructions. Web example 1 evaluation and management (e&m) office visit, blood draw for laboratory screening tests and onsite dispensing of oral contraceptives ‹‹in this example, an established client, who is currently using oral contraceptives, has a history update and a blood pressure check. Cms 1500 field location required field? The center of medicaid and medicare services (cms) form 1500 is used to bill sfhp for medical services. State the type of health insurance applicable to this claim and the insured's id number; This interactive guide provides instruction on how to complete the form.
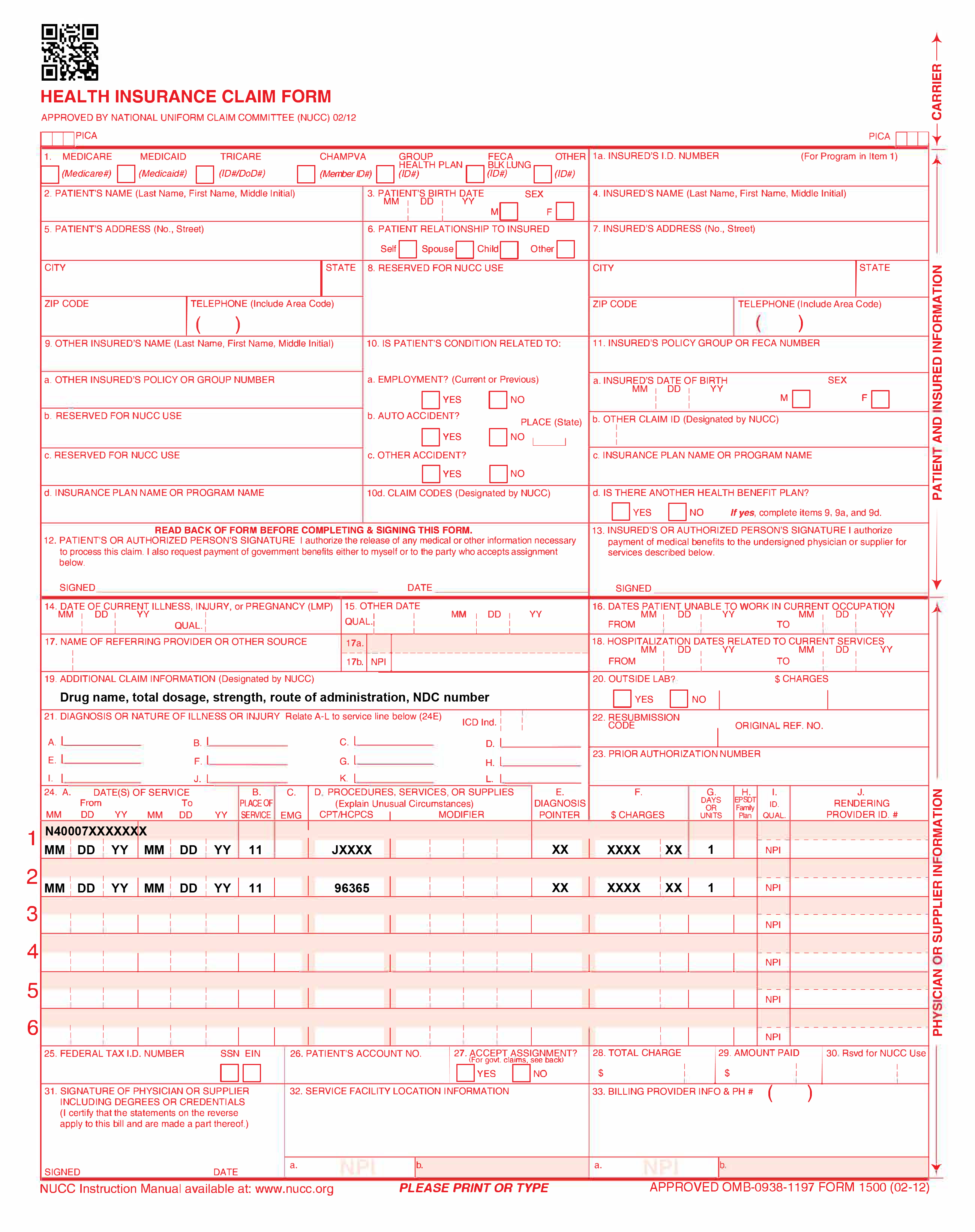
A full year supply of oral contraceptives is dispensed onsite. A cms 1500 with field descriptions and instructions is included in the link below: You'll see instructions on how to complete the field. The form is used by physicians and allied health professionals to submit claims for medical services. You may also click in any field for more detailed instructions. The nucc has developed this general instructions document for completing the 1500claim form. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing requirements as established by the hipaa claim. August 2020 ‹‹legend›› ‹‹symbols used in the document above are explained in the following table.›› symbol description ‹‹ this is a change mark symbol. Insured’s address (no., street) city state zip code telephone (include area code) 11. Billing example for weekly injections.
You may also click in any field for more detailed instructions. All paper claims you submit must be on the appropriate cms claim form. Insured’s policy group or feca number a. Write down the patient's full name, birth date, sex, and address. Required (r) fields must be completed on all claims. Number (for program in item 1) 4. You may also click in any field for more detailed instructions. You'll see instructions on how to complete the field. Web cms 1500 dynamic list information. August 2020 ‹‹legend›› ‹‹symbols used in the document above are explained in the following table.›› symbol description ‹‹ this is a change mark symbol.

Health Insurance Claim Form 1500
Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing requirements as established by the hipaa claim. The patient was seen for an office visit. The cms claim form is available in red ink. This is the only.
Cms 1500 Claim Form Instructions 2016 Form Resume Examples QJ9eN1KYmy
Last updated may 03 , 2022. You can decide how often to. Billing example for weekly injections. You may also click in any field for more detailed instructions. Required (r) fields must be completed on all claims.
New CMS1500 Form (02/12) YouTube
The form is used by physicians and allied health professionals to submit claims for medical services. Write down the patient's full name, birth date, sex, and address. Refer to the nucc website for further detailed instructions. Insured’s address (no., street) city state zip code telephone (include area code) 11. Please adapt to your billing situation.

Example Of Cms 1500 Form Completed Form Resume Examples nO9bvnp94D
Enter the insured's full name, address, and the patient's relationship to the. You can decide how often to. All paper claims you submit must be on the appropriate cms claim form. To ensure timely processing of the claim form, you must follow the form instructions and complete all required information. You may also click in any field for more detailed.
Specialty Drug Resource Sample CMS Forms
In this example, the injection is administered once a week for two weeks. Insured’s name (last name, first name, middle initial) 7. Sign up to get the latest information about your choice of cms topics. You'll see instructions on how to complete the field. The center of medicaid and medicare services (cms) form 1500 is used to bill sfhp for.

Completed Cms 1500 Form Sample Form Resume Examples 9x8raJV3dR
Enter the insured's full name, address, and the patient's relationship to the. Billing example for weekly injections. It should be completed (generally electronically) and submitted to insurance provider in accordance with your organization's policies. This document is intended to be a guide for completing the 1500 claim form and not definitive instructions for this purpose. The center of medicaid and.
Cms 1500 Form Fillable Free Form Resume Examples 1ZV8Bz693X
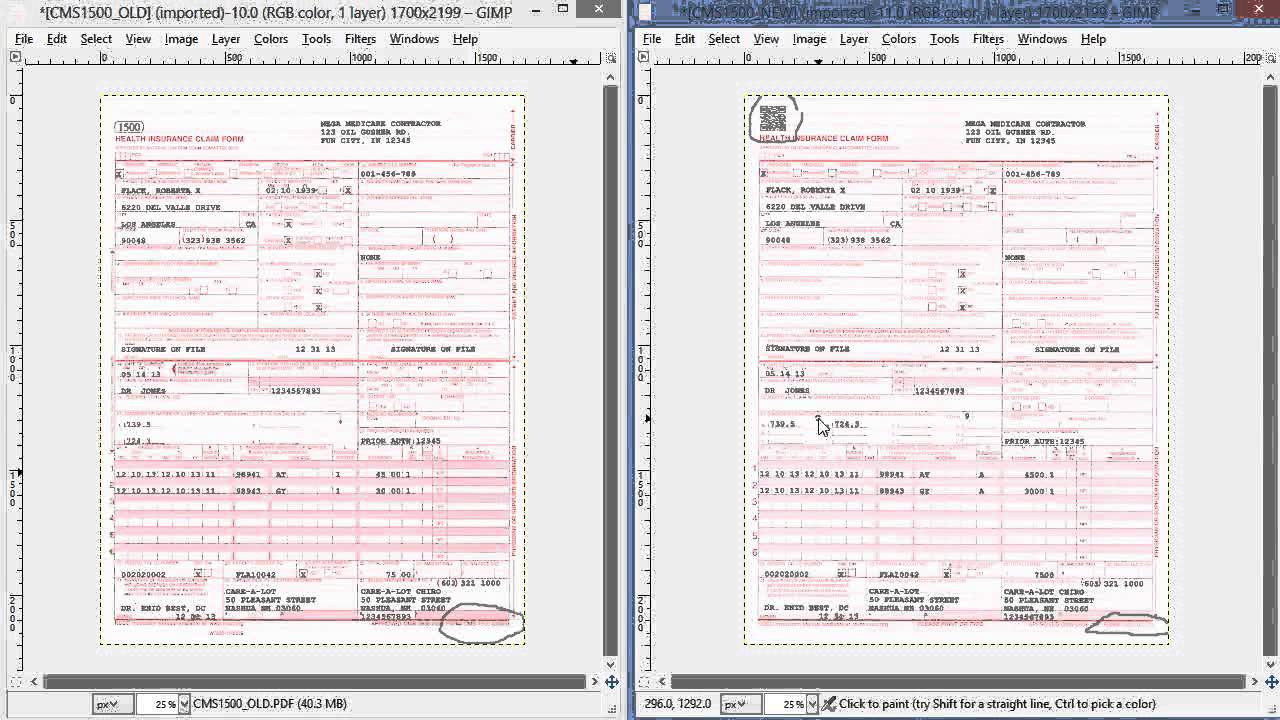
It can be purchased in any version required by calling the u.s. Web the 1500 health insurance claim form (1500 claim form) is in the public domain. The cms claim form is available in red ink. Web coordinated care will only accept the 02/12 version of the cms 1500 (hcfa). Number (for program in item 1) 4.

Cms 1500 Form 0212 Software Universal Network
This interactive guide provides instruction on how to complete the form. Web example 1 evaluation and management (e&m) office visit, blood draw for laboratory screening tests and onsite dispensing of oral contraceptives ‹‹in this example, an established client, who is currently using oral contraceptives, has a history update and a blood pressure check. Insured’s name (last name, first name, middle.
Free Fillable Cms 1500 Template Of Cms 1500 form Pdf Free Claim form
You'll see instructions on how to complete the field. Web the 1500 health insurance claim form (1500 claim form) is in the public domain. A cms 1500 with field descriptions and instructions is included in the link below: State the type of health insurance applicable to this claim and the insured's id number; Claims may be electronically submitted to a.

Form Cms 1500 Instructions Form Resume Examples Wk9y1XX93D
Insured’s policy group or feca number a. The center of medicaid and medicare services (cms) form 1500 is used to bill sfhp for medical services. Last updated wed, 04 jan 2023 13:36:02 +0000. Web coordinated care will only accept the 02/12 version of the cms 1500 (hcfa). A cms 1500 with field descriptions and instructions is included in the link.
Web Medicare Claims Processing Manual.
Cms 1500 field location required field? Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing requirements as established by the hipaa claim. In this example, the injection is administered once a week for two weeks. Web coordinated care will only accept the 02/12 version of the cms 1500 (hcfa).
A Cms 1500 With Field Descriptions And Instructions Is Included In The Link Below:
Tufts does not want the new form until april 1, 2014. The form is used by physicians and allied health professionals to submit claims for medical services. Insured’s address (no., street) city state zip code telephone (include area code) 11. You'll see instructions on how to complete the field.
The Cms Claim Form Is Available In Red Ink.
The patient was seen for an office visit. Insured’s name (last name, first name, middle initial) 7. Required (r) fields must be completed on all claims. This interactive guide provides instruction on how to complete the form.
Sign Up To Get The Latest Information About Your Choice Of Cms Topics.
State the type of health insurance applicable to this claim and the insured's id number; This is a sample only. Web cms 1500 dynamic list information. Billing example for weekly injections.