Flu Shot Verification Form
Flu Shot Verification Form - Web health care personnel influenza vaccination form am a va: Web keeping an immunization record and storing it with other important documents (or in a safe place) will save you time and unnecessary hassle. Web adult vaccination records. Influenza is a serious respiratory disease. This section includes suggestions for collecting personal and demographic information. Trainee, resident, intern, fee basis, or researcher) please indicate: To be completed by the student influenza verification form last name:first name: Do not have any of the conditions listed below: How to locate your vaccination records; What to do if you can’t find your records;
Tools to record your vaccinations. Ask your doctor, pharmacist or other vaccine provider for an immunization record form or download and use this form [4 pages]. Influenza vaccine is strongly recommended for healthcare workers, not only to protect themselves, but to reduce the change of spreading influenza to the patients and community. Web keeping an immunization record and storing it with other important documents (or in a safe place) will save you time and unnecessary hassle. Flu test vaccine consent form. Do not have any of the conditions listed below: Trainee, resident, intern, fee basis, or researcher) please indicate: Web this record can be in electronic or paper form. Flu vaccine consent form template. This section includes suggestions for collecting personal and demographic information.
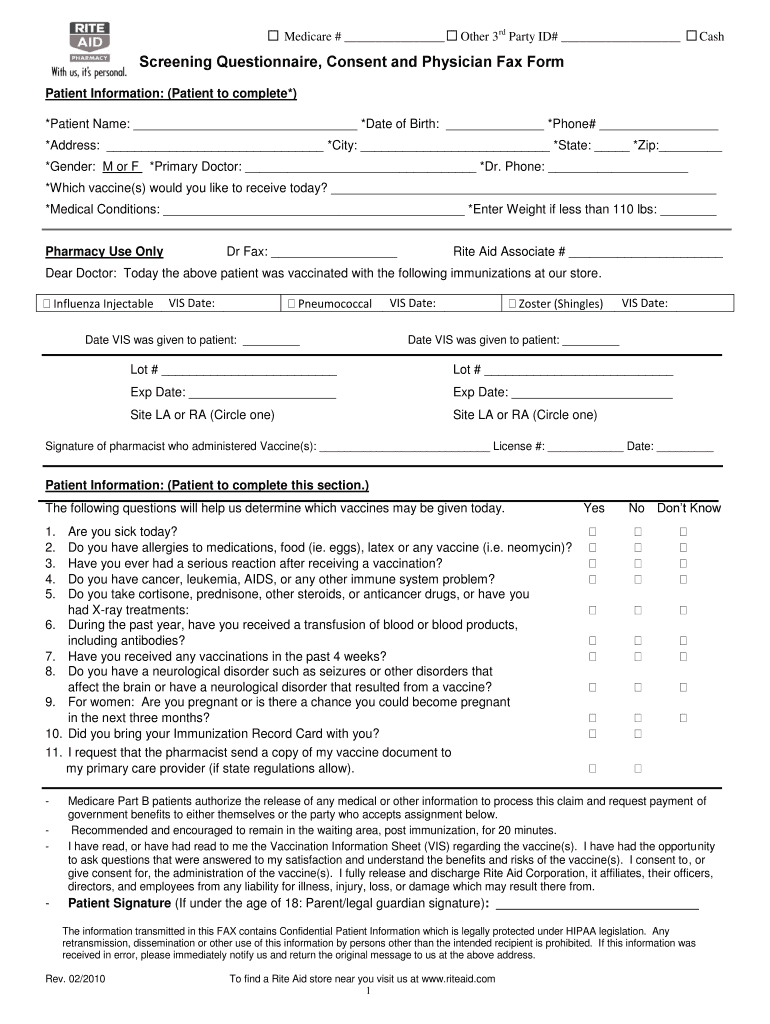
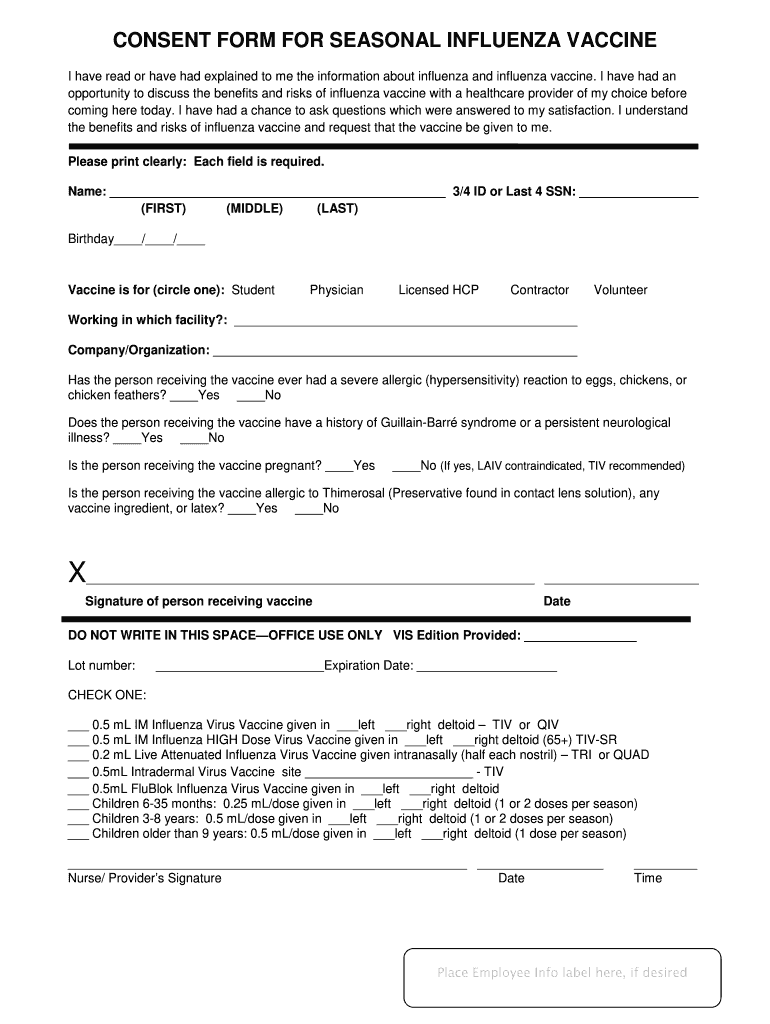
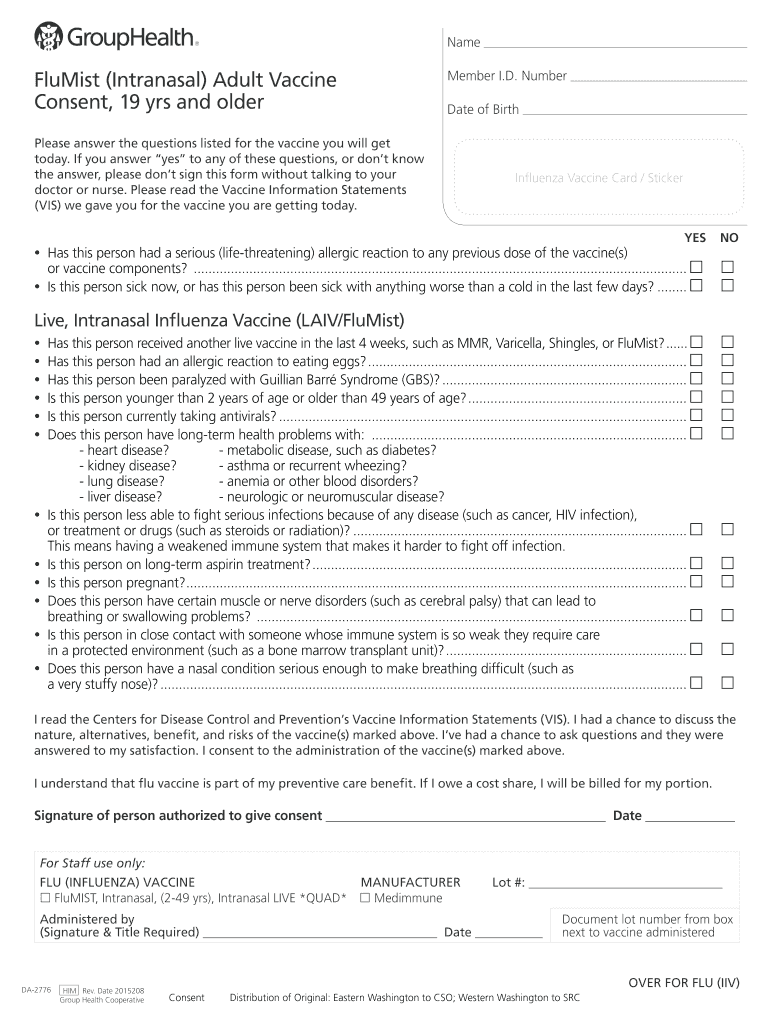
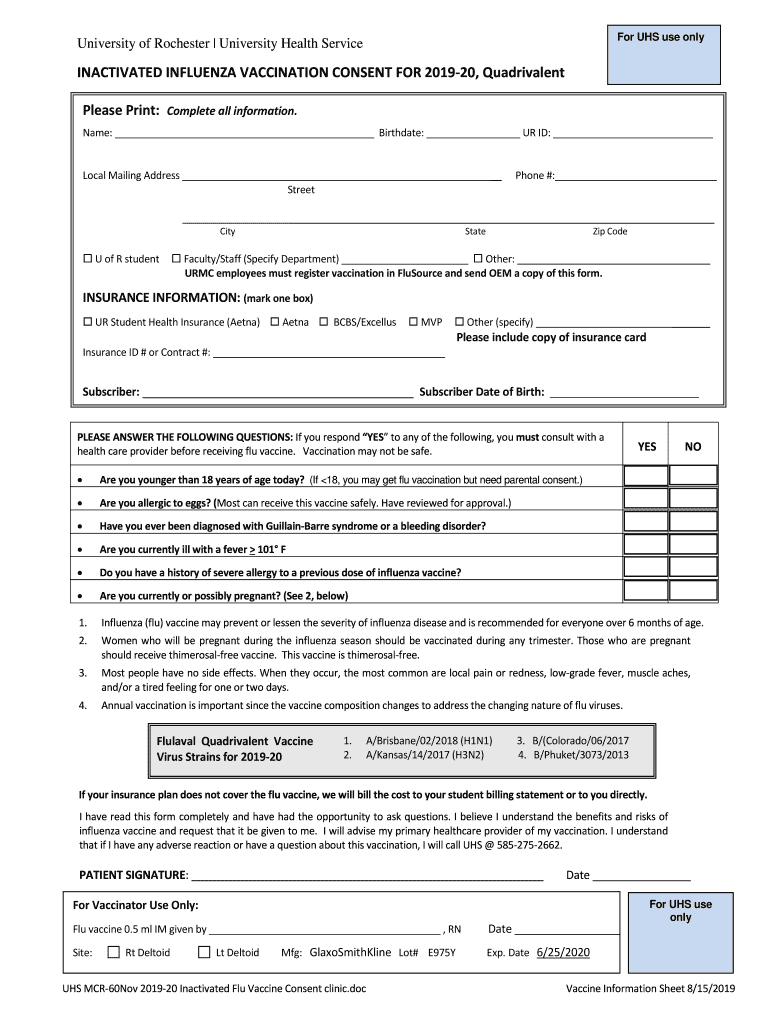
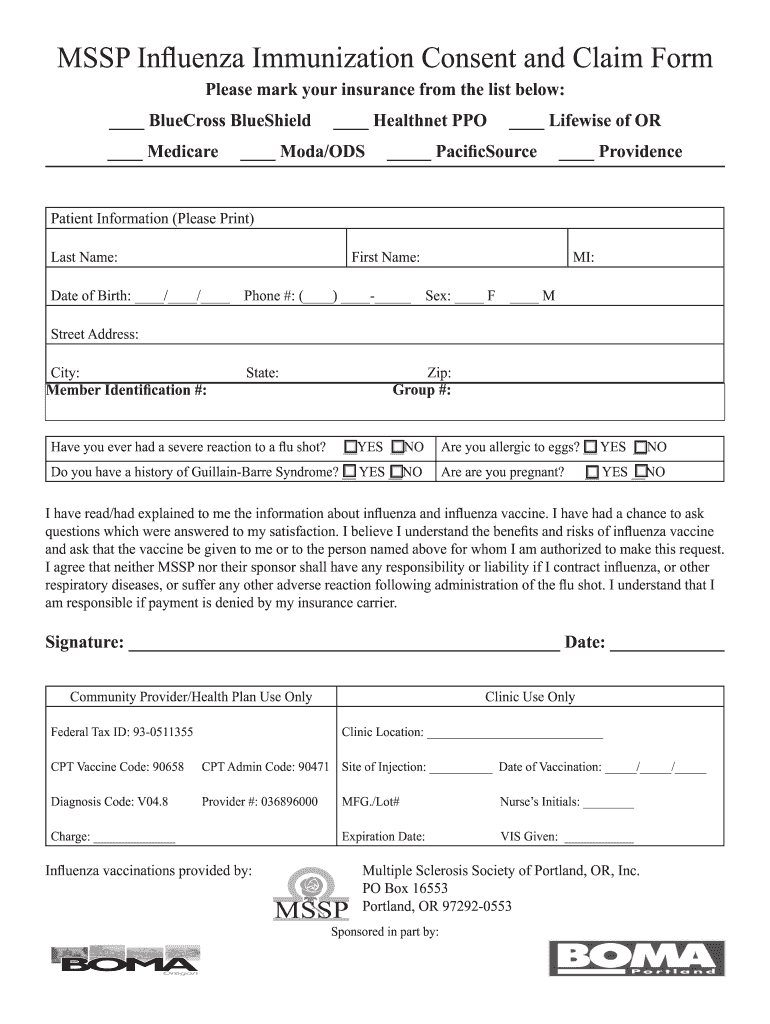
Date of administration vaccine manufacturer vaccine lot number This section includes suggestions for collecting personal and demographic information. Web download our free templates and simplify the process of obtaining consent for flu vaccinations. Flu vaccine consent form template. Check one statement below and complete and sign the last section of this form prior to submission to employee occupational health: Influenza is a serious respiratory disease. It should be signed by the patient, or, in the case of a minor, by a parent or legal guardian. Health care providers who administer vaccines covered by the national childhood vaccine injury act are required to ensure that the permanent medical record of the recipient indicates: To be completed by the student influenza verification form last name:first name: Serious reaction to previous flu vaccine.

Buy fluverificationpanel (Product Code NATFVPNNS) Life Science
Web adult vaccination records. What to do if you can’t find your records; Web health care personnel influenza vaccination form am a va: Web download our free templates and simplify the process of obtaining consent for flu vaccinations. Do not have any of the conditions listed below:

Flu Shot Proof Form Form Resume Examples J3DW4am5Lp
Health care providers who administer vaccines covered by the national childhood vaccine injury act are required to ensure that the permanent medical record of the recipient indicates: Flu vaccine consent form template. Do not have any of the conditions listed below: Web this record can be in electronic or paper form. Web influenza vaccination verification form influenza vaccination verification form.
Document 13194918
Flu vaccine consent form template. Tools to record your vaccinations. Web download our free templates and simplify the process of obtaining consent for flu vaccinations. Web keeping an immunization record and storing it with other important documents (or in a safe place) will save you time and unnecessary hassle. Below are notes about each section on the template consent forms:
Printable Flu Shot Verification Form Printable Word Searches
To be completed by the student influenza verification form last name:first name: Check one statement below and complete and sign the last section of this form prior to submission to employee occupational health: What to do if you can’t find your records; Fillable influenza vaccination consent form. Ask your doctor, pharmacist or other vaccine provider for an immunization record form.
Flu Shot Form Fill Out and Sign Printable PDF Template signNow
Tools to record your vaccinations. How to locate your vaccination records; What to do if you can’t find your records; Serious reaction to previous flu vaccine. Michigan influenza vaccination consent form.
Pneumonia Vaccine Consent Form Fill Out and Sign Printable PDF
Web this record can be in electronic or paper form. Web influenza vaccination verification form influenza vaccination verification form columbus public health recommends that anyone without medical contraindications receive an influenza vaccination annually to protect themselves, their families and the public. Check one statement below and complete and sign the last section of this form prior to submission to employee.

Flu Shot Verification Form Form Resume Examples yKVBbNLoVM
Web this record can be in electronic or paper form. Web influenza vaccination verification form influenza vaccination verification form columbus public health recommends that anyone without medical contraindications receive an influenza vaccination annually to protect themselves, their families and the public. Check one statement below and complete and sign the last section of this form prior to submission to employee.
Influenza Flu 20 Vaccine Consent Form University of Fill Out and Sign
Influenza is a serious respiratory disease. Michigan influenza vaccination consent form. Health care providers who administer vaccines covered by the national childhood vaccine injury act are required to ensure that the permanent medical record of the recipient indicates: Web this record can be in electronic or paper form. How to locate your vaccination records;
Printable Flu Shot Verification Form Printable Word Searches
Michigan influenza vaccination consent form. Influenza is a serious respiratory disease. Tools to record your vaccinations. Web influenza vaccination verification form influenza vaccination verification form columbus public health recommends that anyone without medical contraindications receive an influenza vaccination annually to protect themselves, their families and the public. Date of administration vaccine manufacturer vaccine lot number
Free Flu Shot (Influenza) Vaccine Consent Form PDF Word eForms
Influenza vaccine is strongly recommended for healthcare workers, not only to protect themselves, but to reduce the change of spreading influenza to the patients and community. Flu vaccine consent form template. Tools to record your vaccinations. Trainee, resident, intern, fee basis, or researcher) please indicate: Web this record can be in electronic or paper form.
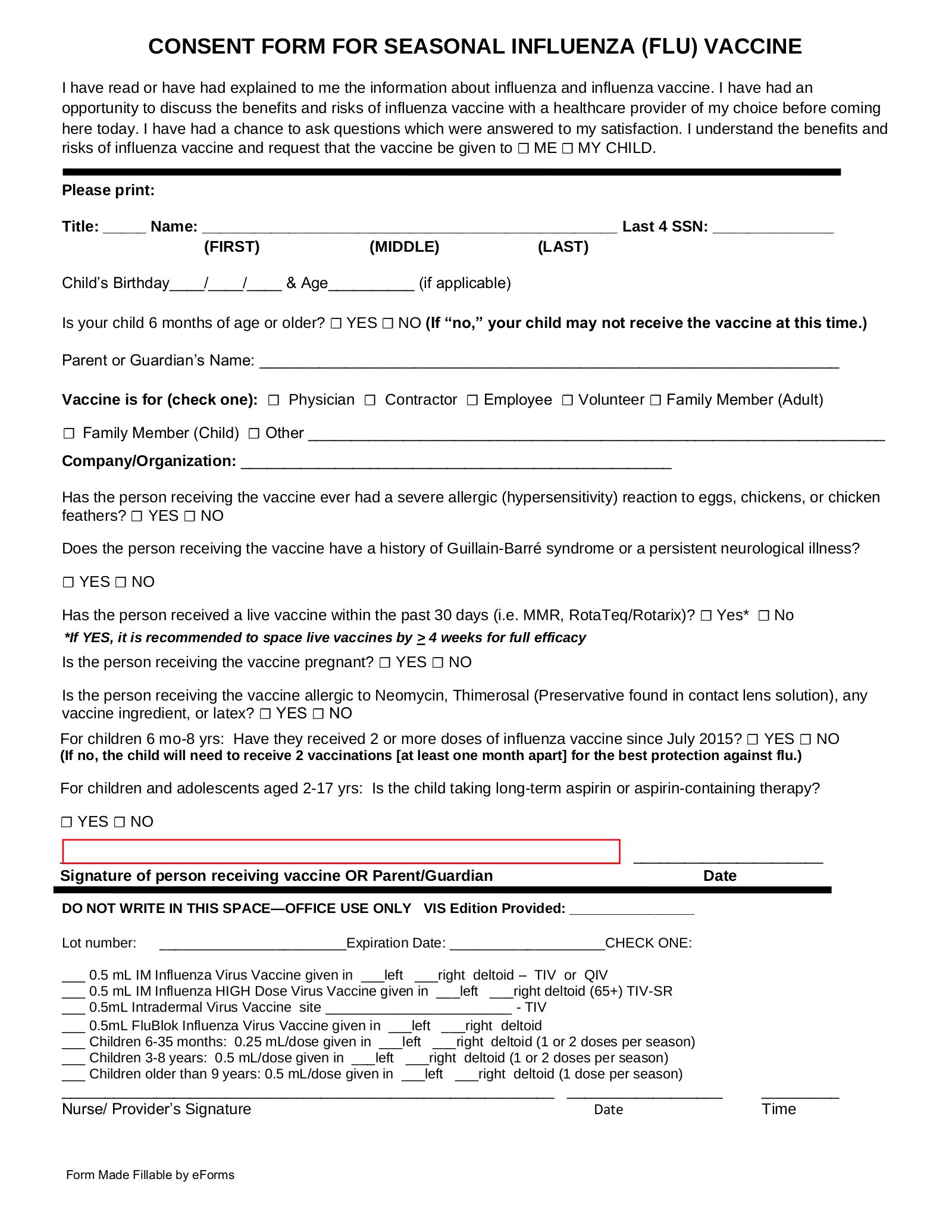
It Should Be Signed By The Patient, Or, In The Case Of A Minor, By A Parent Or Legal Guardian.
Trainee, resident, intern, fee basis, or researcher) please indicate: Web adult vaccination records. Web this record can be in electronic or paper form. How to locate your vaccination records;
What To Do If You Can’t Find Your Records;
To be completed by the student influenza verification form last name:first name: Serious reaction to previous flu vaccine. Ask your doctor, pharmacist or other vaccine provider for an immunization record form or download and use this form [4 pages]. Below are notes about each section on the template consent forms:
Information About Child To Receive Vaccine:
Web keeping an immunization record and storing it with other important documents (or in a safe place) will save you time and unnecessary hassle. Influenza vaccine is strongly recommended for healthcare workers, not only to protect themselves, but to reduce the change of spreading influenza to the patients and community. Do not have any of the conditions listed below: Health care providers who administer vaccines covered by the national childhood vaccine injury act are required to ensure that the permanent medical record of the recipient indicates:
Check One Statement Below And Complete And Sign The Last Section Of This Form Prior To Submission To Employee Occupational Health:
Date of administration vaccine manufacturer vaccine lot number Influenza is a serious respiratory disease. This section includes suggestions for collecting personal and demographic information. Web health care personnel influenza vaccination form am a va: