Free Printable Medical Records Request Form
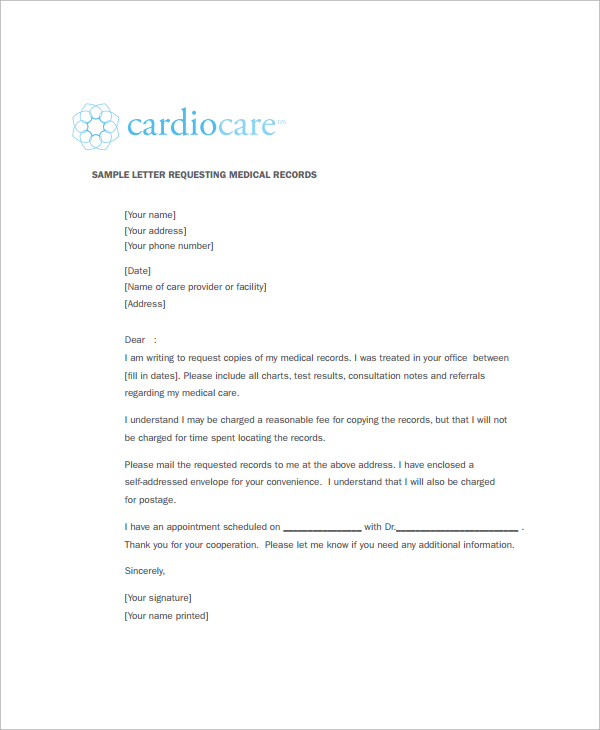
Free Printable Medical Records Request Form - Patients should consider the recipient and the information required when selecting a. Complete the document answer a few questions and your document is created automatically. A medical records release (hipaa) form is a written authorization for health providers to release information to the patient and someone other than the patient. A medical release form can be revoked or reassigned at any time by the patient. It also describes the types of information that can be shared without your consent and how to make corrections. The federal health insurance portability and accountability act of 1996 (hipaa) and state laws mandate that health. The release also allows the added option for healthcare providers to share information. Web the medical record information release (hipaa) form allows a patient to give authorization to a 3rd party and access their health records. Choose this template start by clicking on fill out the template 2. Web this article explains how to make a request for medical records and what to do if a request is denied.
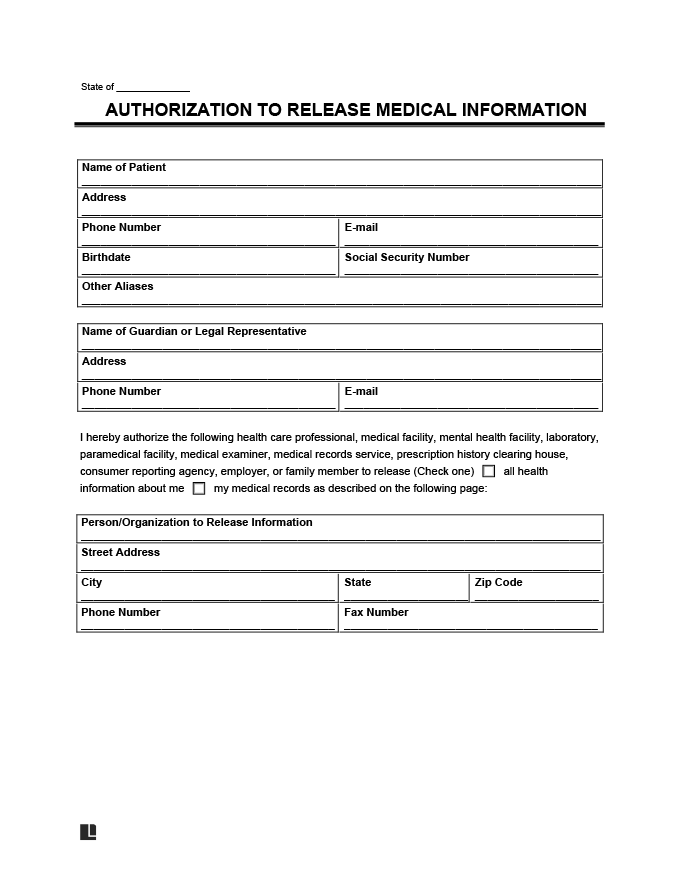
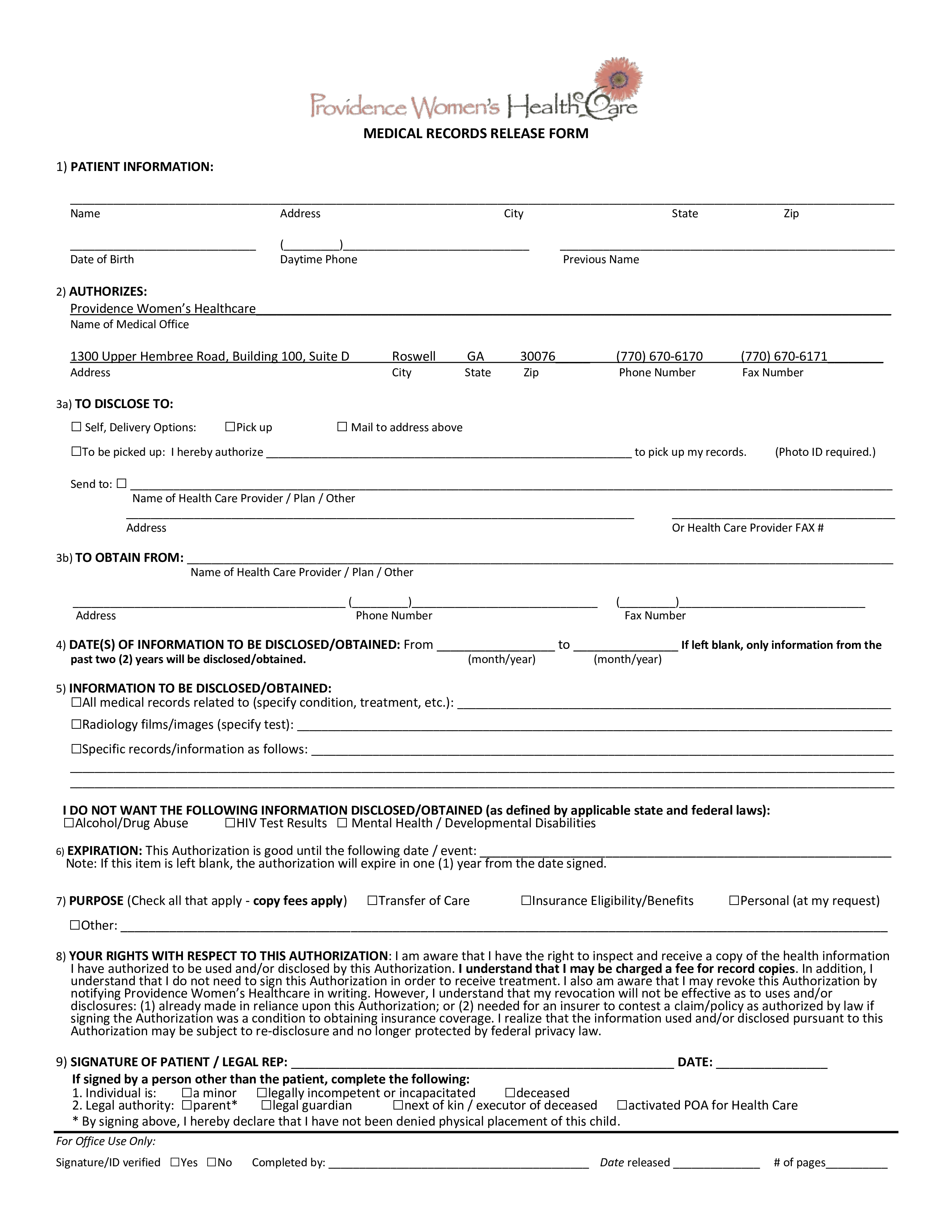
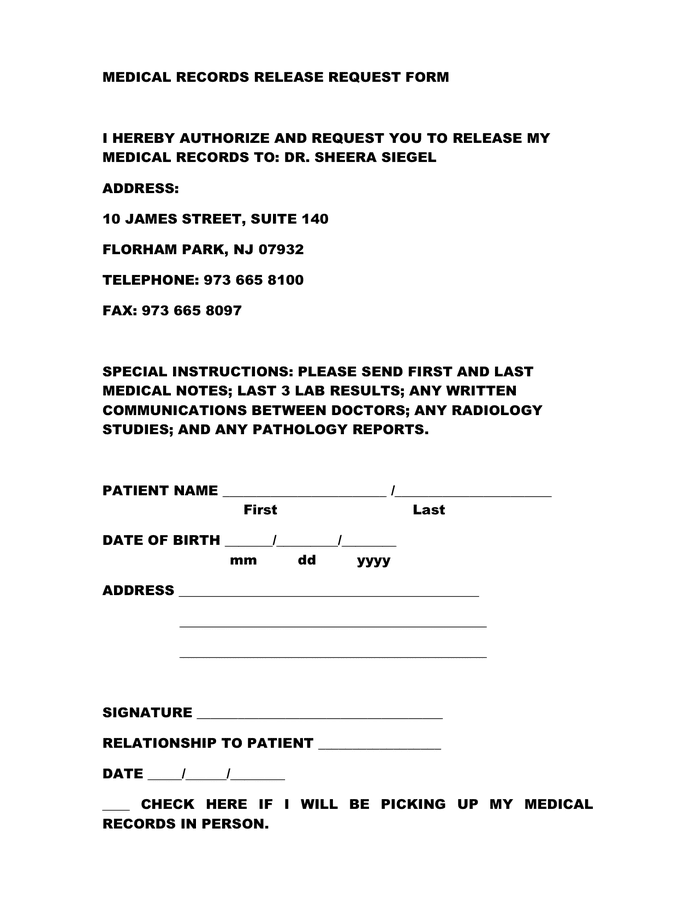
Web updated july 27, 2023 | legally reviewed by susan chai, esq. If you're a mayo clinic health system patient or have been one in the past, you can use these forms to grant permission for others to access your protected health information or request a change to your health record. The federal health insurance portability and accountability act of 1996 (hipaa) and state laws mandate that health. Web to request release of medical information please complete and sign this form i, _____hereby voluntarily authorize the disclosure of information from my health record. Choose this template start by clicking on fill out the template 2. (name of patient) patient information: Web this article explains how to make a request for medical records and what to do if a request is denied. A medical records release (hipaa) form is a written authorization for health providers to release information to the patient and someone other than the patient. Complete the document answer a few questions and your document is created automatically. It also describes the types of information that can be shared without your consent and how to make corrections.
The federal health insurance portability and accountability act of 1996 (hipaa) and state laws mandate that health. It also describes the types of information that can be shared without your consent and how to make corrections. You will receive it in word and pdf formats. Choose this template start by clicking on fill out the template 2. Web updated july 27, 2023 | legally reviewed by susan chai, esq. A medical records release (hipaa) form is a written authorization for health providers to release information to the patient and someone other than the patient. Patients should consider the recipient and the information required when selecting a. A medical release form can be revoked or reassigned at any time by the patient. Web to request release of medical information please complete and sign this form i, _____hereby voluntarily authorize the disclosure of information from my health record. (name of patient) patient information:
Medical Records Release (HIPAA) Form PDF & Word Legal Templates
Choose this template start by clicking on fill out the template 2. A medical release form can be revoked or reassigned at any time by the patient. Web choosing the best type of hipaa form is important to authorize an individual, medical professional, billing office, or insurance representative to release or view medical records. The release also allows the added.
Printable Medical Records Release Form Templates at
Choose this template start by clicking on fill out the template 2. It also describes the types of information that can be shared without your consent and how to make corrections. Patients should consider the recipient and the information required when selecting a. Web the medical record information release (hipaa) form allows a patient to give authorization to a 3rd.
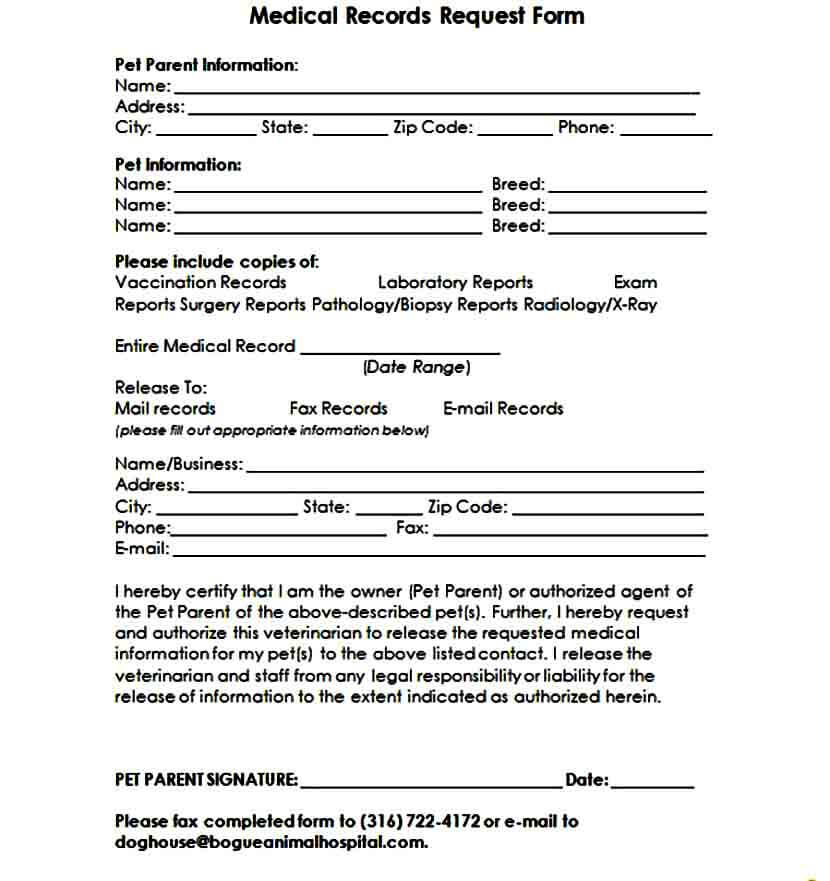
FREE 12+ Medical Records Request Forms in PDF Word
Web updated july 27, 2023 | legally reviewed by susan chai, esq. Complete the document answer a few questions and your document is created automatically. If you're a mayo clinic health system patient or have been one in the past, you can use these forms to grant permission for others to access your protected health information or request a change.

blank medical records release form Medical records, Medical, Doctors
Web this article explains how to make a request for medical records and what to do if a request is denied. A medical release form can be revoked or reassigned at any time by the patient. Complete the document answer a few questions and your document is created automatically. You will receive it in word and pdf formats. It also.
Medical records release request form in Word and Pdf formats
A medical release form can be revoked or reassigned at any time by the patient. Choose this template start by clicking on fill out the template 2. Patients should consider the recipient and the information required when selecting a. Web choosing the best type of hipaa form is important to authorize an individual, medical professional, billing office, or insurance representative.
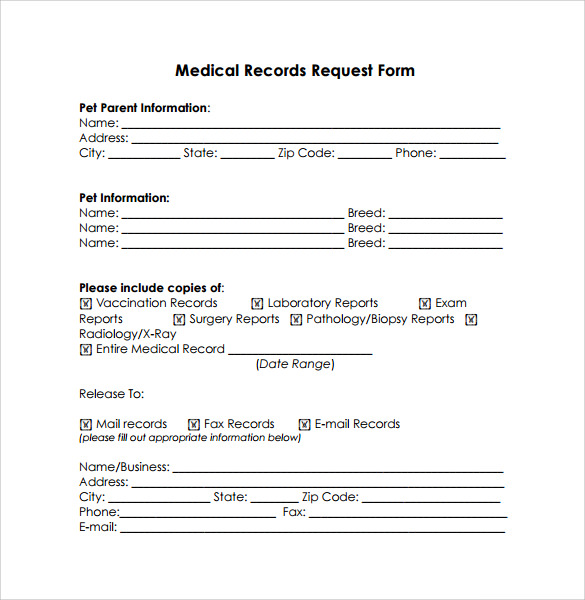
Blank Medical Records Release Form amulette
Web the medical record information release (hipaa) form allows a patient to give authorization to a 3rd party and access their health records. Choose this template start by clicking on fill out the template 2. You will be able to modify it. It also describes the types of information that can be shared without your consent and how to make.
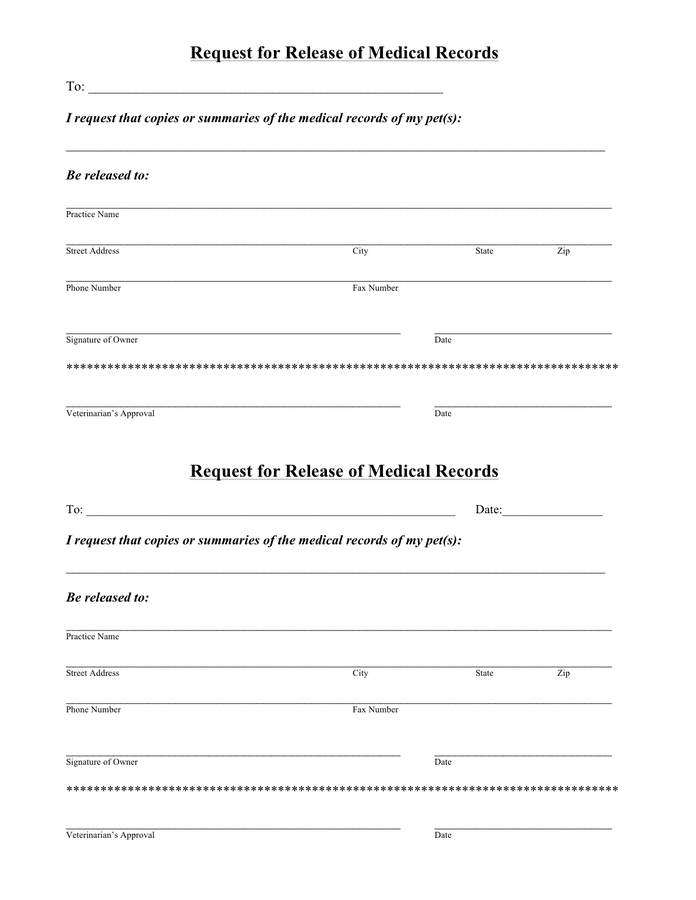
Hospital Request Form for Release of Medical Records in Word and Pdf
Web the medical record information release (hipaa) form allows a patient to give authorization to a 3rd party and access their health records. A medical release form can be revoked or reassigned at any time by the patient. Web updated july 27, 2023 | legally reviewed by susan chai, esq. Web to request release of medical information please complete and.
Sample Medical Records Release Form Mous Syusa
A medical release form can be revoked or reassigned at any time by the patient. Choose this template start by clicking on fill out the template 2. Web this article explains how to make a request for medical records and what to do if a request is denied. The federal health insurance portability and accountability act of 1996 (hipaa) and.
FREE 10+ Medical Records Release Forms in PDF
Web the medical record information release (hipaa) form allows a patient to give authorization to a 3rd party and access their health records. Complete the document answer a few questions and your document is created automatically. Patients should consider the recipient and the information required when selecting a. The release also allows the added option for healthcare providers to share.
Medical Records Release Form templates free printable
The federal health insurance portability and accountability act of 1996 (hipaa) and state laws mandate that health. Web updated july 27, 2023 | legally reviewed by susan chai, esq. Complete the document answer a few questions and your document is created automatically. Web this article explains how to make a request for medical records and what to do if a.
Web Choosing The Best Type Of Hipaa Form Is Important To Authorize An Individual, Medical Professional, Billing Office, Or Insurance Representative To Release Or View Medical Records.
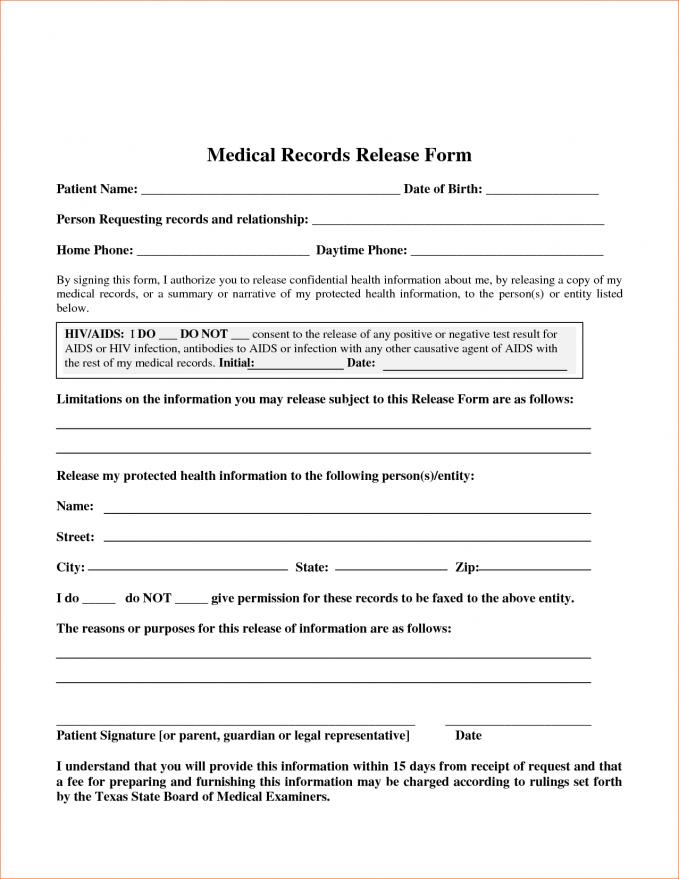
A medical records release (hipaa) form is a written authorization for health providers to release information to the patient and someone other than the patient. Patients should consider the recipient and the information required when selecting a. You will be able to modify it. Web updated july 27, 2023 | legally reviewed by susan chai, esq.
Web To Request Release Of Medical Information Please Complete And Sign This Form I, _____Hereby Voluntarily Authorize The Disclosure Of Information From My Health Record.
The federal health insurance portability and accountability act of 1996 (hipaa) and state laws mandate that health. Web this article explains how to make a request for medical records and what to do if a request is denied. You will receive it in word and pdf formats. Web the medical record information release (hipaa) form allows a patient to give authorization to a 3rd party and access their health records.
Choose This Template Start By Clicking On Fill Out The Template 2.
If you're a mayo clinic health system patient or have been one in the past, you can use these forms to grant permission for others to access your protected health information or request a change to your health record. (name of patient) patient information: It also describes the types of information that can be shared without your consent and how to make corrections. Complete the document answer a few questions and your document is created automatically.
A Medical Release Form Can Be Revoked Or Reassigned At Any Time By The Patient.
The release also allows the added option for healthcare providers to share information.