Hipaa Authorization Form Michigan
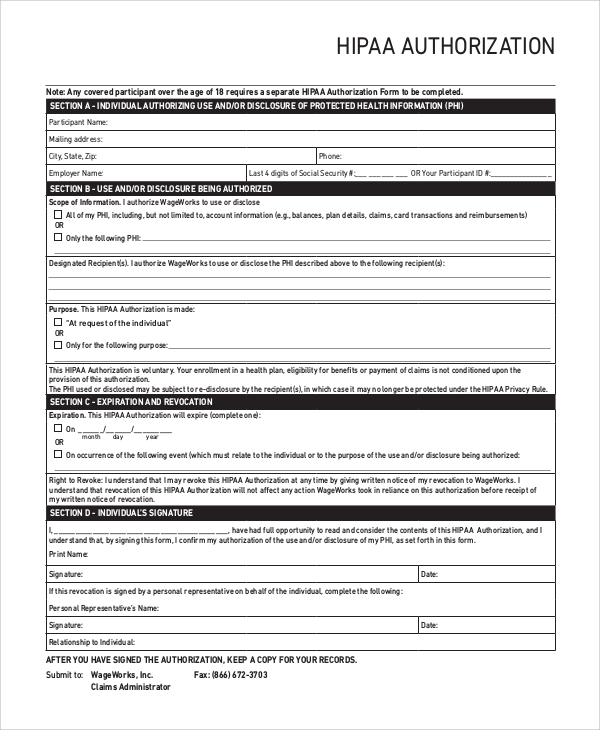
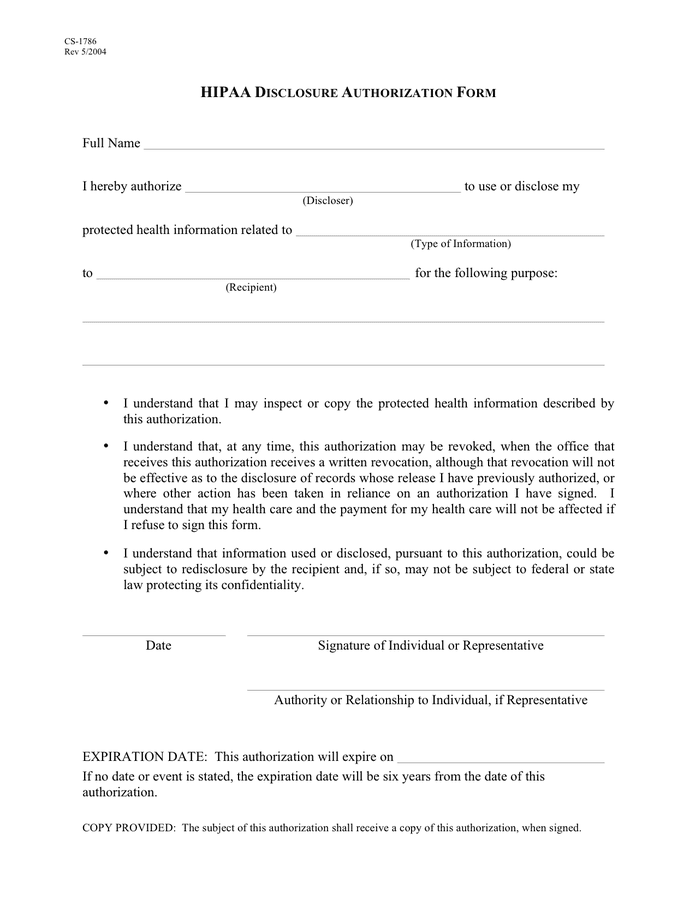
Hipaa Authorization Form Michigan - An individual's rights under hipaa authorization to disclose protected health information (recipient) i understand that i may inspect or copy the protected health information described by this authorization. Web doing business with mdhhs health care providers hipaa an individual's rights under hipaa hipaa privacy and the individual's power to exercise their rights. All other uses and disclosures require your prior written authorization. Authorization for disclosure of protected health information birth date: I authorize and request sparrow health system (or ) to use or make a disclosure of my protected health information (phi), including, without limitation, my name and the following, as applicable: Web i am the patient, or the legally authorized representative of the patient listed above and request michigan medicine to authorization to release copies of a medical record (patient requests information to be sent from umhs) for clinic use only: Web hipaa disclosure authorization form full name i hereby authorize to use or disclose my (discloser) protected health information related to (type of information) to for the following purpose: To disclose to third parties on the request of the individual or a personal representative of the individual. Hipaa regulations outline the uses and disclosures of phi that require authorization to be obtained from a patient/plan member before that person’s phi can be shared or used.
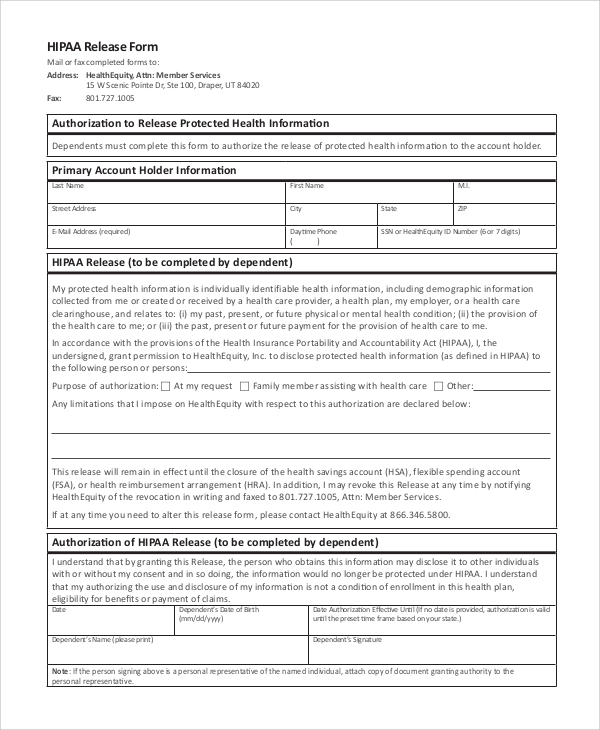
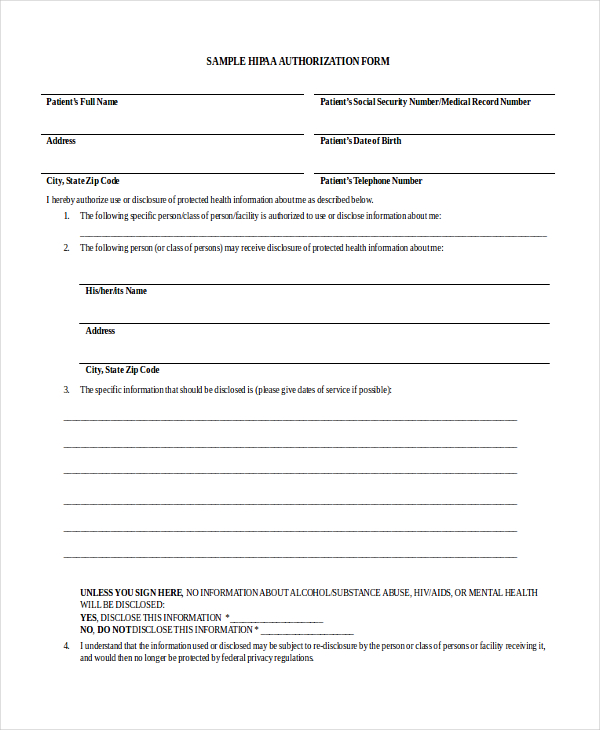
Sale of phi psychotherapy notes. Web michigan law and/or federal regulations place certain additional restrictions on the use and disclosure of phi for mental health, substance abuse, hiv/aids conditions, and certain genetic information. To disclose to third parties on the request of the individual or a personal representative of the individual. This form is acceptable to the michigan department of health and human services as compliant with hipaa privacy regulations, 45cfr parts 160 and 164 as modified august 14, 2002. Hipaa regulations outline the uses and disclosures of phi that require authorization to be obtained from a patient/plan member before that person’s phi can be shared or used. Web doing business with mdhhs health care providers hipaa an individual's rights under hipaa hipaa privacy and the individual's power to exercise their rights. Web the following uses and disclosures require a signed hipaa compliant authorization: Web use this form to authorize blue cross blue shield of michigan, blue care network, blue care network service company, blue care of michigan, inc. Web i am the patient, or the legally authorized representative of the patient listed above and request michigan medicine to authorization to release copies of a medical record (patient requests information to be sent from umhs) for clinic use only: Is voluntary, but required if.
(recipient) i understand that i may inspect or copy the protected health information described by this authorization. And/or blue cross complete of michigan to disclose your protected health information to. Web michigan law and/or federal regulations place certain additional restrictions on the use and disclosure of phi for mental health, substance abuse, hiv/aids conditions, and certain genetic information. Authorization for disclosure of protected health information birth date: An individual's rights under hipaa authorization to disclose protected health information In some instances, your specific authorization may be required. Web doing business with mdhhs health care providers hipaa an individual's rights under hipaa hipaa privacy and the individual's power to exercise their rights. Web i am the patient, or the legally authorized representative of the patient listed above and request michigan medicine to authorization to release copies of a medical record (patient requests information to be sent from umhs) for clinic use only: Is voluntary, but required if. Web use this form to authorize blue cross blue shield of michigan, blue care network, blue care network service company, blue care of michigan, inc.
33 INFO SAMPLE HIPAA FORM DOWNLOAD PDF DOC ZIP Interview
I authorize and request sparrow health system (or ) to use or make a disclosure of my protected health information (phi), including, without limitation, my name and the following, as applicable: An individual's rights under hipaa authorization to disclose protected health information Web doing business with mdhhs health care providers hipaa an individual's rights under hipaa hipaa privacy and the.
FREE 8+ Sample Hipaa Release Forms in PDF MS Word
In some instances, your specific authorization may be required. An individual's rights under hipaa authorization to disclose protected health information Web michigan law and/or federal regulations place certain additional restrictions on the use and disclosure of phi for mental health, substance abuse, hiv/aids conditions, and certain genetic information. Web doing business with mdhhs health care providers hipaa an individual's rights.
FREE 9+ Sample Hipaa Forms in PDF MS Word
All other uses and disclosures require your prior written authorization. I understand that i may inspect or copy the protected health information described by this authorization. An individual's rights under hipaa authorization to disclose protected health information Web hipaa authorization form michigan a hipaa authorization form in michigan is required under certain circumstances. This form is acceptable to the michigan.
Hipaa Authorization To Release Medical Information Form Arizona
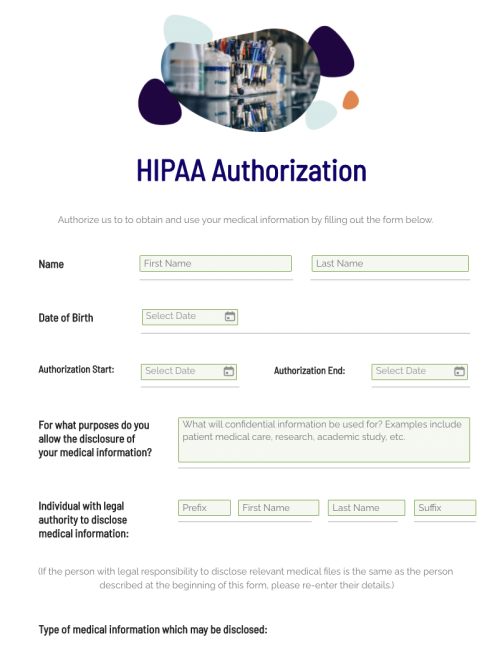
Is voluntary, but required if. An individual's rights under hipaa authorization to disclose protected health information Web hipaa disclosure authorization form full name i hereby authorize to use or disclose my (discloser) protected health information related to (type of information) to for the following purpose: Web the following uses and disclosures require a signed hipaa compliant authorization: In some instances,.
FREE 11+ Sample HIPAA Forms in PDF MS Word
Click here for access to privacy right request and complaint forms. Web michigan law and/or federal regulations place certain additional restrictions on the use and disclosure of phi for mental health, substance abuse, hiv/aids conditions, and certain genetic information. Web hipaa disclosure authorization form full name i hereby authorize to use or disclose my (discloser) protected health information related to.
HIPAA Disclosure Authorization Form Michigan in Word and Pdf formats
Sale of phi psychotherapy notes. Authorization for disclosure of protected health information birth date: Web the following uses and disclosures require a signed hipaa compliant authorization: Web michigan law and/or federal regulations place certain additional restrictions on the use and disclosure of phi for mental health, substance abuse, hiv/aids conditions, and certain genetic information. All other uses and disclosures require.
Free HIPAA Authorization Form Fill Out 2022 Template
I understand that i may inspect or copy the protected health information described by this authorization. Web use this form to authorize blue cross blue shield of michigan, blue care network, blue care network service company, blue care of michigan, inc. All other uses and disclosures require your prior written authorization. Web i am the patient, or the legally authorized.
When & Why You Need a HIPAA Authorization Form Abyde
I understand that i may inspect or copy the protected health information described by this authorization. In some instances, your specific authorization may be required. Hipaa regulations outline the uses and disclosures of phi that require authorization to be obtained from a patient/plan member before that person’s phi can be shared or used. Web use this form to authorize blue.
Free Medical Records Release Authorization Form HIPAA Word PDF
In some instances, your specific authorization may be required. Web hipaa authorization form michigan a hipaa authorization form in michigan is required under certain circumstances. Authorization for disclosure of protected health information birth date: Is voluntary, but required if. And/or blue cross complete of michigan to disclose your protected health information to.

HIPAA Disclosure Authorization Form Michigan in Word and Pdf formats
Web hipaa disclosure authorization form full name i hereby authorize to use or disclose my (discloser) protected health information related to (type of information) to for the following purpose: Hipaa regulations outline the uses and disclosures of phi that require authorization to be obtained from a patient/plan member before that person’s phi can be shared or used. And/or blue cross.
To Disclose To Third Parties On The Request Of The Individual Or A Personal Representative Of The Individual.
Sale of phi psychotherapy notes. And/or blue cross complete of michigan to disclose your protected health information to. Web hipaa authorization form michigan a hipaa authorization form in michigan is required under certain circumstances. An individual's rights under hipaa authorization to disclose protected health information
This Form Is Acceptable To The Michigan Department Of Health And Human Services As Compliant With Hipaa Privacy Regulations, 45Cfr Parts 160 And 164 As Modified August 14, 2002.
When individual admits to a crime when requesting treatment, or while in treatment, except as required by law. Is voluntary, but required if. Web the following uses and disclosures require a signed hipaa compliant authorization: Web hipaa disclosure authorization form full name i hereby authorize to use or disclose my (discloser) protected health information related to (type of information) to for the following purpose:
I Understand That I May Inspect Or Copy The Protected Health Information Described By This Authorization.
(recipient) i understand that i may inspect or copy the protected health information described by this authorization. Web michigan law and/or federal regulations place certain additional restrictions on the use and disclosure of phi for mental health, substance abuse, hiv/aids conditions, and certain genetic information. Hipaa regulations outline the uses and disclosures of phi that require authorization to be obtained from a patient/plan member before that person’s phi can be shared or used. Web use this form to authorize blue cross blue shield of michigan, blue care network, blue care network service company, blue care of michigan, inc.
Web I Am The Patient, Or The Legally Authorized Representative Of The Patient Listed Above And Request Michigan Medicine To Authorization To Release Copies Of A Medical Record (Patient Requests Information To Be Sent From Umhs) For Clinic Use Only:
All other uses and disclosures require your prior written authorization. I authorize and request sparrow health system (or ) to use or make a disclosure of my protected health information (phi), including, without limitation, my name and the following, as applicable: Click here for access to privacy right request and complaint forms. Authorization for disclosure of protected health information birth date: