Molina Appeal Form
Molina Appeal Form - Web instructions for filing a complaint/appeal: Web if you call us to request a quick appeal, you do not need to send molina this form. State administrative hearing step 3: Describe the issue(s) in as much detail as possible. Local time, 7 days a week. You may submit the completed form through one of. Health care authority (hca) board of appeals review judge decision how do i ask for (file) an appeal? Important information you need to know if you are unhappy with the steps we and/or your doctor took for your request, let. Fill out this form completely. Web member grievance/appeal request form molina healthcare cannot promise that the way in which you submit this form to us is a secured method.
Important information you need to know if you are unhappy with the steps we and/or your doctor took for your request, let. Molina healthcare standard and expedited appeal step 2: Please include a copy of the eob with the appeal and any supporting documentation. Thank you for using the molina healthcare member grievance & appeal process. Web provider claims appeal request form provider information: Web if you call us to request a quick appeal, you do not need to send molina this form. Web member grievance/appeal request form molina healthcare cannot promise that the way in which you submit this form to us is a secured method. Web instructions for filing a complaint/appeal: Molina healthcare of texas attention: State administrative hearing step 3:
Web instructions for filing a complaint/appeal: You may submit the completed form through one of. Box 165089 irving, tx 75016 member grievance/appeal request form molina healthcare recognizes the fact that members may not always be satisfied with the care and services provided by our contracted doctors, hospitals and other providers. Appeals & grievances department, 5232 witz drive, north syracuse, ny 13212. Appeals & grievances department or by mail to molina healthcare of new york, attention: Fill out this form completely. Health care authority (hca) board of appeals review judge decision how do i ask for (file) an appeal? Molina healthcare standard and expedited appeal step 2: Important information you need to know if you are unhappy with the steps we and/or your doctor took for your request, let. Attach copies of any records you wish to submit.

Medicaid Appeal Form Virginia Form Resume Examples
Appeals & grievances department or by mail to molina healthcare of new york, attention: Health care authority (hca) board of appeals review judge decision how do i ask for (file) an appeal? Web contact us select your state from the menu below: Molina healthcare of texas attention: Box 165089 irving, tx 75016 member grievance/appeal request form molina healthcare recognizes the.

Molina contributes to Cards win; will appeal suspension
Please include a copy of the eob with the appeal and any supporting documentation. Appeals & grievances department or by mail to molina healthcare of new york, attention: Web member grievance/appeal request form molina healthcare cannot promise that the way in which you submit this form to us is a secured method. State administrative hearing step 3: Box 165089 irving,.

Going to the Source The Molina Letter, A Spaniard's Appeal to Stop
☐ inquiry appeal tax id: Fill out this form completely. We want to know about your problems and complaints. Box 165089 irving, tx 75016 # of pages (including caf cover sheet) date: Local time, 7 days a week.

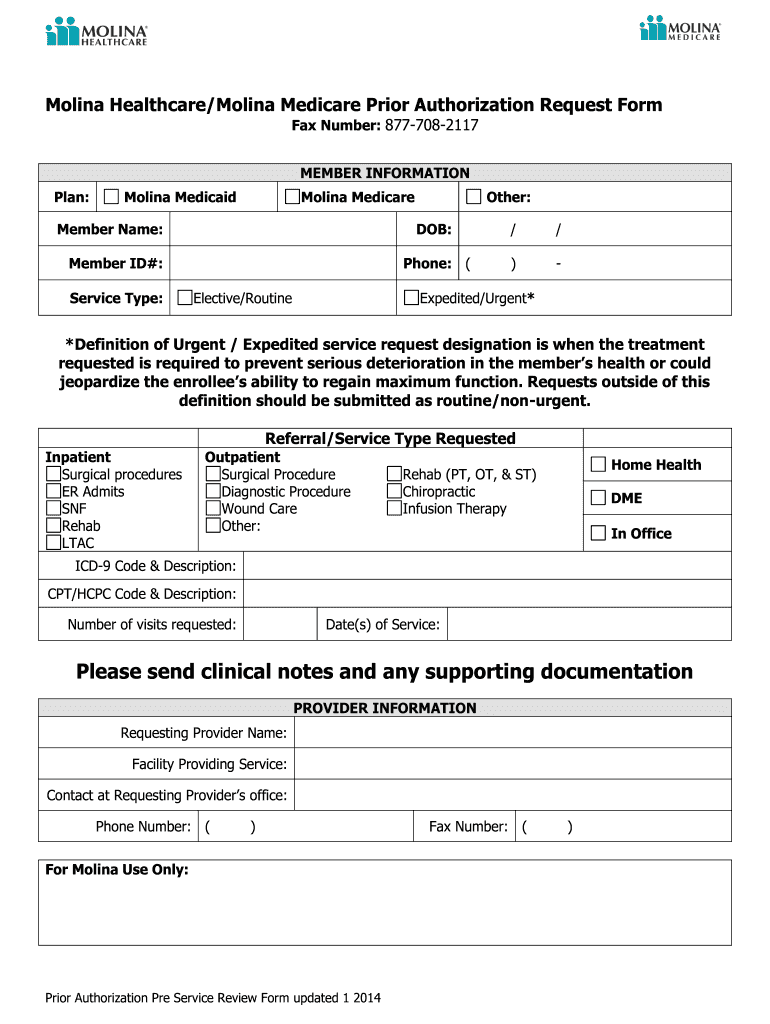
ads/responsive.txt Molina Healthcare Prior Authorization form New
Local time, 7 days a week. Attach copies of any records you wish to submit. Web instructions for filing a complaint/appeal: Web provider claims appeal request form provider information: Important information you need to know if you are unhappy with the steps we and/or your doctor took for your request, let.

Molina Medicare Pa Forms Universal Network
We want to know about your problems and complaints. Local time, 7 days a week. Box 165089 irving, tx 75016 # of pages (including caf cover sheet) date: Molina healthcare of texas attention: Thank you for using the molina healthcare member grievance & appeal process.
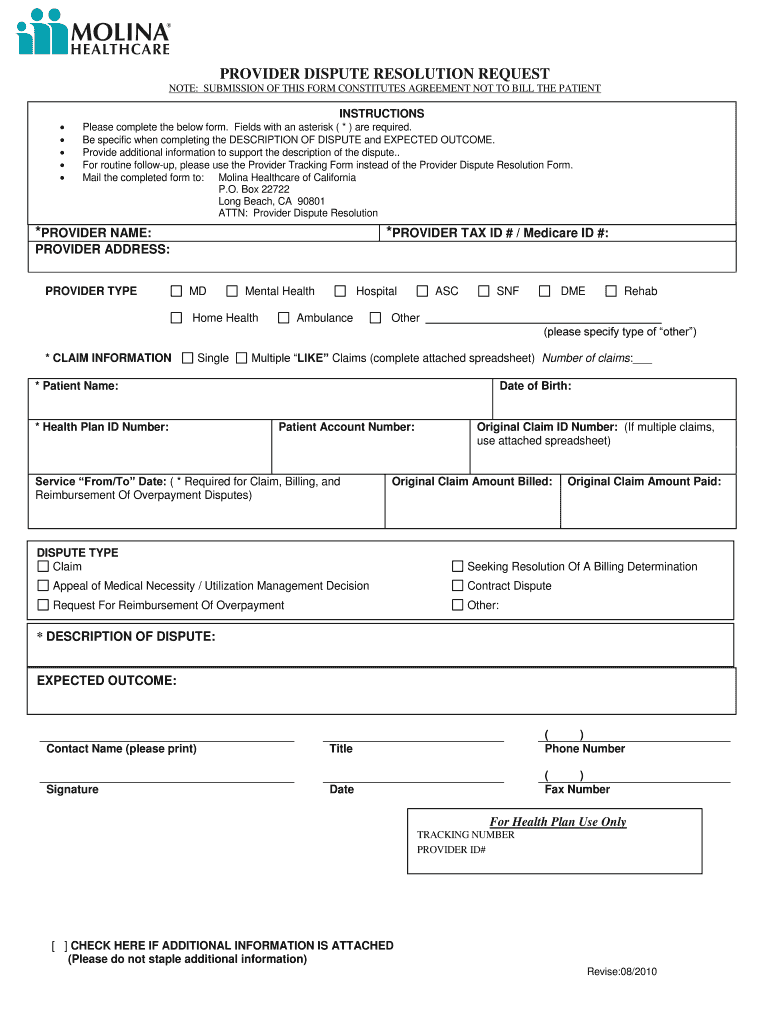
Molina provider dispute resolution form Fill out & sign online DocHub
Attach copies of any records you wish to submit. State administrative hearing step 3: Web instructions for filing a complaint/appeal: Please include a copy of the eob with the appeal and any supporting documentation. Appeals & grievances department or by mail to molina healthcare of new york, attention:

Washington Molina Marketplace Appeal Request Form. Washington Molina
State administrative hearing step 3: ☐ inquiry appeal tax id: Member healthcare provider denied service: You may submit the completed form through one of. Appeals & grievances department, 5232 witz drive, north syracuse, ny 13212.
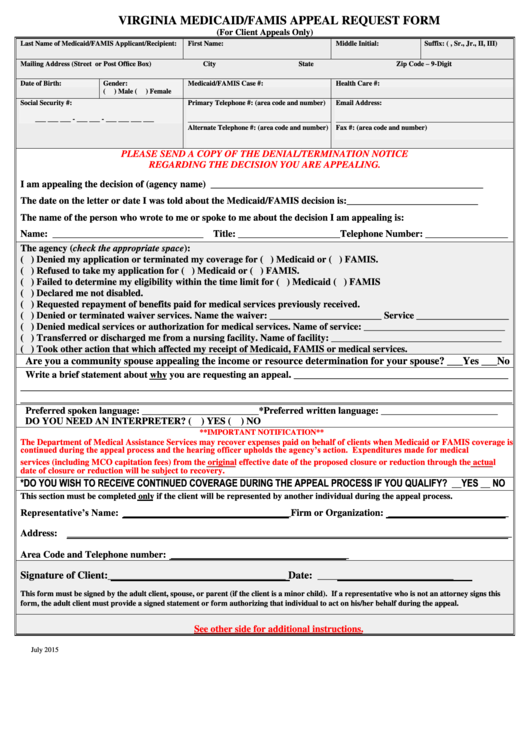
Virginia Medicaid/famis Appeal Request Form printable pdf download
Molina healthcare of texas attention: ☐ inquiry appeal tax id: You may submit the completed form through one of. Important information you need to know if you are unhappy with the steps we and/or your doctor took for your request, let. Web if you call us to request a quick appeal, you do not need to send molina this form.
Molina Prior Authorization Form Fill Out and Sign Printable PDF
Web provider claims appeal request form provider information: ☐ inquiry appeal tax id: Member healthcare provider denied service: Molina healthcare of texas attention: Web contact us select your state from the menu below:

WA Molina Healthcare Behavioral Health Authorization/Notification Form
☐ inquiry appeal tax id: Attach copies of any records you wish to submit. State administrative hearing step 3: Web member grievance/appeal request form molina healthcare cannot promise that the way in which you submit this form to us is a secured method. Appeals & grievances department or by mail to molina healthcare of new york, attention:
Web If You Call Us To Request A Quick Appeal, You Do Not Need To Send Molina This Form.
Appeals & grievances department, 5232 witz drive, north syracuse, ny 13212. ☐ inquiry appeal tax id: Describe the issue(s) in as much detail as possible. Thank you for using the molina healthcare member grievance & appeal process.
Box 165089 Irving, Tx 75016 # Of Pages (Including Caf Cover Sheet) Date:
Box 165089 irving, tx 75016 member grievance/appeal request form molina healthcare recognizes the fact that members may not always be satisfied with the care and services provided by our contracted doctors, hospitals and other providers. Attach copies of any records you wish to submit. Local time, 7 days a week. Web instructions for filing a complaint/appeal:
Important Information You Need To Know If You Are Unhappy With The Steps We And/Or Your Doctor Took For Your Request, Let.
State administrative hearing step 3: Web provider claims appeal request form provider information: Molina healthcare of texas attention: Health care authority (hca) board of appeals review judge decision how do i ask for (file) an appeal?
Appeals & Grievances Department Or By Mail To Molina Healthcare Of New York, Attention:
Web contact us select your state from the menu below: We want to know about your problems and complaints. Web member grievance/appeal request form molina healthcare cannot promise that the way in which you submit this form to us is a secured method. Please include a copy of the eob with the appeal and any supporting documentation.