Numc Medical Records Request Form
Numc Medical Records Request Form - To request a copy of your medical record, please download and complete the request for access to health information form. Medical records 2790 clay edwards drive north kansas city, mo 64116 fax: If any section is not complete or section 5 unsigned, this authorization will be considered incomplete and not. Web i or my personal representative hereby request that northwell health provide access to my health information as described in this form. Web accessing my medical records; Web we propose diagnosis and treatment in over 70 technical and subspecialties, as well when programs, services, press support the assist you stay well throughout your lifetime. North kansas city hospital attn: Web access my medical records; Learn how to request medical records from an atlantic health system hospital. Medical records requests must be made to the facility where care took place (a hospital or physician’s office).
For other questions, call 816.691.1587 and select option 2. Medical records requests must be made to the facility where care took place (a hospital or physician’s office). We contact healthcare providers on your behalf. Web make an appointment | access my medical records | refill my prescription insurance access If records are needed by more than one person/facility, a separate request is required. Understand and use these rights. To request a copy of your medical record, please download and complete the request for access to health information form. Web we help you request your medical records, get driving directions, find contact numbers, and read independent reviews. Download the form in english ; If records are requested for personal reasons, a fee may be charged.
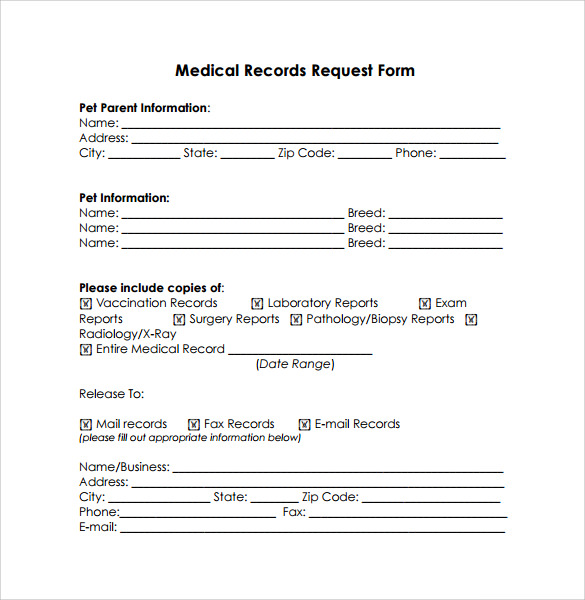
There should only be one patient listed on the form. Learn about in centers from care; For other questions, call 816.691.1587 and select option 2. Web we help you request your medical records, get driving directions, find contact numbers, and read independent reviews. Web we propose diagnosis and treatment in over 70 technical and subspecialties, as well when programs, services, press support the assist you stay well throughout your lifetime. Download this release of information authorization form, and fill it out: Medical records 2790 clay edwards drive north kansas city, mo 64116 fax: Download the form in spanish ; If records are requested for personal reasons, a fee may be charged. North kansas city hospital attn:

Request Archives Page 2 of 4 PDFSimpli
Learn about in centers from care; For other questions, call 816.691.1587 and select option 2. Learn how to request medical records from an atlantic health system hospital. We contact your healthcare providers on your behalf, just request your records from any healthcare provider in the us, using our convenient hipaa compliant online process and we will provide you quickly and.

NUMC is 2017 Business of the Year News, Sports, Jobs The Journal
Web what you need to know. Web need access to your medical records? Thanking a staff member or physician; Web to get your medical records from nassau university medical center. Download the form in english ;
Sample Medical Records Release Form Mous Syusa
Complete a simple secure form. If records are requested for personal reasons, a fee may be charged. Web we help you request your medical records, get driving directions, find contact numbers, and read independent reviews. Web make an appointment | access my medical records | refill my prescription insurance access Web what you need to know.
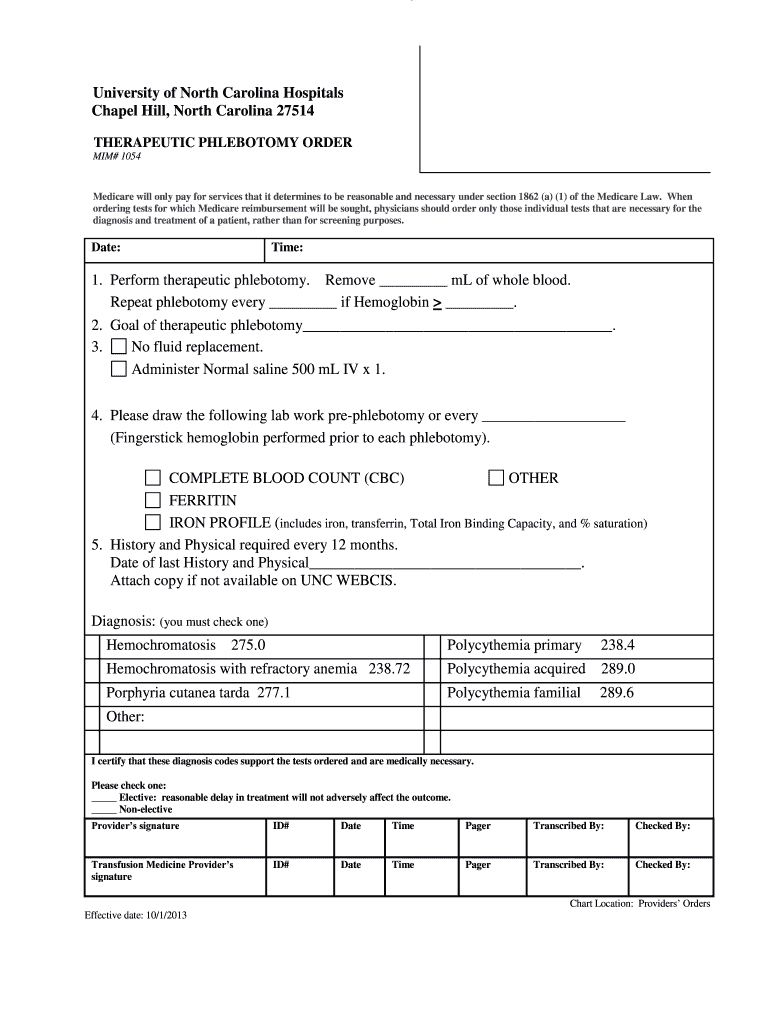
Therapeutic Phlebotomy Guidelines Pdf Fill Out and Sign Printable PDF
Web home / patients & visitors / patient bill of rights patient bill of rights as a patient in a hospital in new york state, you have the right, consistent with law, to: Web access my medical records; Complete a simple secure form. Web learn how to request medizinischen records coming an atlantic health system hospital. Web accessing my medical.
Medical Records Request Form in Word and Pdf formats
Web i or my personal representative hereby request that northwell health provide access to my health information as described in this form. Download the form in english ; Understand and use these rights. Web there is no charge for sending medical records directly to another medical facility or doctor. Learn about in centers from care;

Download Texas Medical Records Request Form for Free FormTemplate
If records are needed by more than one person/facility, a separate request is required. Download the form in spanish ; Medical records 2790 clay edwards drive north kansas city, mo 64116 fax: Web make an appointment | gain mys medical records | refill my prescription insurance access Download this release of information authorization form, and fill it out:

Medical Records Request Form Khatoon Dehwar
Learn learn our organizational of care; Learn how to request medical records from an atlantic health system hospital. Web accessing my medical records; Download this release of information authorization form, and fill it out: We contact your healthcare providers on your behalf, just request your records from any healthcare provider in the us, using our convenient hipaa compliant online process.
FREE 10+ Medical Records Release Forms in PDF
Web need access to your medical records? We contact healthcare providers on your behalf. Web medical records | northwell health. Download the form in english ; Web there is no charge for sending medical records directly to another medical facility or doctor.
Medical records request form in Word and Pdf formats
Nmc health’s health information management (him) department is available to help you get copies of your file. Download the form in spanish ; Web access my medical records; We contact your healthcare providers on your behalf, just request your records from any healthcare provider in the us, using our convenient hipaa compliant online process and we will provide you quickly.

Download Medical Records Request Form for Free FormTemplate
There should only be one patient listed on the form. Medical records requests must be made to the facility where care took place (a hospital or physician’s office). To request a copy of your medical record, please download and complete the request for access to health information form. Download the form in spanish ; We contact healthcare providers on your.
Download This Release Of Information Authorization Form, And Fill It Out:
To request printed or electronic copies of your nmc health medical records, fill out and sign our release of information form. Give ampere staff member or physician; For other questions, call 816.691.1587 and select option 2. Web need access to your medical records?
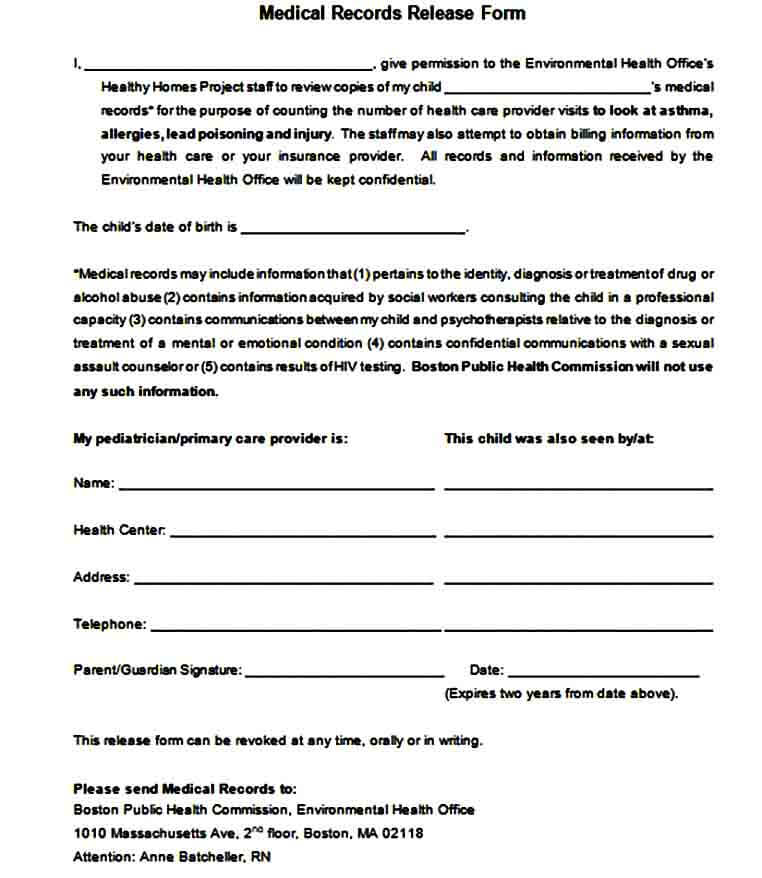
Medical Record Abstract (Summary Of Record) £ Medical Record From (Insert Date) ______________ To (Insert Date) ______________ £ Entire Medical Record £ Laboratory Results For Date Of Service ______________ £ Radiology Images And Reports For Date Of Service ______________ £
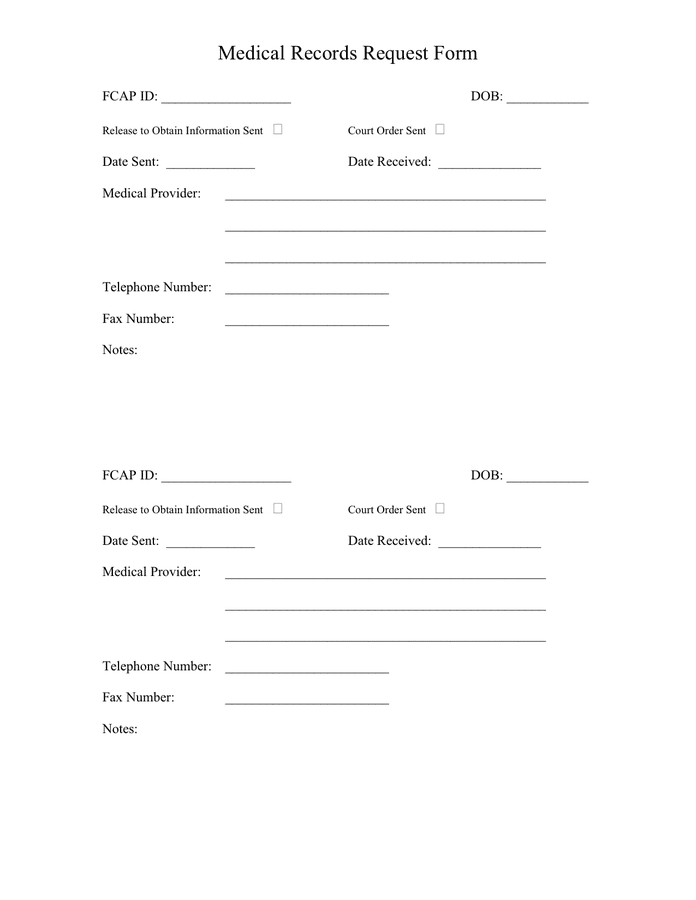
Thanking a staff member or physician; Web enter the name, date of birth, address, and telephone number of the patient requesting records. Web accessing my medical records; Download the form in english ;
Complete A Simple Secure Form.
If any section is not complete or section 5 unsigned, this authorization will be considered incomplete and not. Learn about in centers from care; Web i or my personal representative hereby request that northwell health provide access to my health information as described in this form. Medical records 2790 clay edwards drive north kansas city, mo 64116 fax:
I Am Making This Request Under The Provisions Of The Health Insurance Portability And Accountability
Finish an authorization for the release of information gestalt. Web make an appointment | gain mys medical records | refill my prescription insurance access If records are requested for personal reasons, a fee may be charged. Web medical records | northwell health.