Upmc Appeal Form
Upmc Appeal Form - Web upmc for life members may ask for a coverage determination or redetermination (appeal) for a part d prescription drug. Web if so, you’ll need to submit an “appointment of representative” form [pdf, 47.7kb]. Web every upmc patient can request a change to their medical record if they believe there's incorrect or incomplete information. Web for home and community based service providers. Web signed release form/consent form must have a signature (electronic accepted) within a 12 month time period of submission cahq is not accepted/supported by upmc refunds. Ad patients travel from around the world for our nationally recognized care. Web upmc encourages patients to apply for financial assistance if they believe that they are unable to pay all or part of their upmc bill. Use the links below to learn more. We’re proud to provide the best care to those who rely on us every day. Web when the body sends immune cells to the muscles, this causes inflammation.
2 only clean claims containing the required information will be processed within the required time limits. Web how to contact us if you have any questions about this document or would like to make an appeal or complaint about your medical care or part d prescription drugs: Web to ask for a coverage determination, redetermination, or appeal about a part d drug, a signed, written request should be faxed to upmc health plan or sent to the address. If ohma doesn't issue a timely decision, you may ask omha to move your case to the. Over time, the muscles get weak. Ad patients travel from around the world for our nationally recognized care. Web in fact, back pain is common. Web download the authorization for the release of protected health information form (pdf). Web when the body sends immune cells to the muscles, this causes inflammation. Web upmc encourages patients to apply for financial assistance if they believe that they are unable to pay all or part of their upmc bill.
Over time, the muscles get weak. Consent for treatment, payment and health care operations. Upmc shadyside family health center. Sign and date the form. Medicaid eligibility changes will impact all medicaid recipients. To request a change, fill out the upmc patient. Web upmc, a nonprofit corp.; Use the links below to learn more. Web every upmc patient can request a change to their medical record if they believe there's incorrect or incomplete information. Web when the body sends immune cells to the muscles, this causes inflammation.
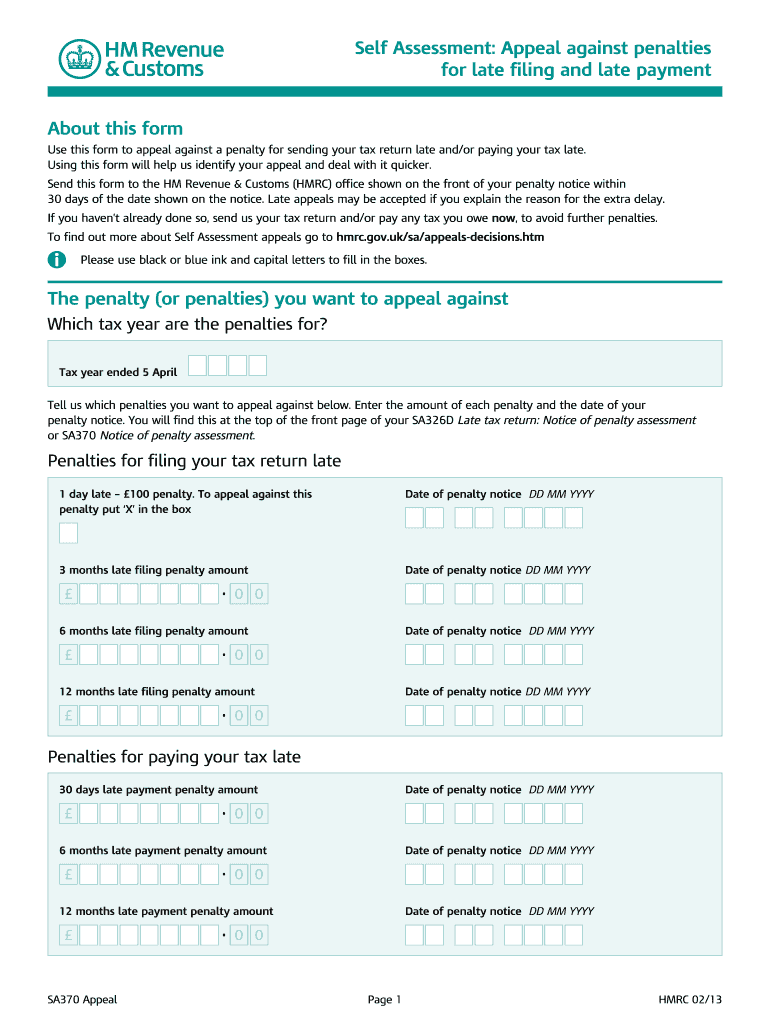
Sa370 Appeal Form Fill Online, Printable, Fillable, Blank PDFfiller
Web when the body sends immune cells to the muscles, this causes inflammation. Web how to contact us if you have any questions about this document or would like to make an appeal or complaint about your medical care or part d prescription drugs: Web • please submit a separate form for each claim (this guide should not be submitted.

Upmc Dependent Tuition Assistance Request Form
Web how to contact us if you have any questions about this document or would like to make an appeal or complaint about your medical care or part d prescription drugs: Web if so, you’ll need to submit an “appointment of representative” form [pdf, 47.7kb]. We’re proud to provide the best care to those who rely on us every day..

Grade Appeal Form
If ohma doesn't issue a timely decision, you may ask omha to move your case to the. Web signed release form/consent form must have a signature (electronic accepted) within a 12 month time period of submission cahq is not accepted/supported by upmc refunds. Medicaid eligibility changes will impact all medicaid recipients. Upmc shadyside family health center. Web download the authorization.
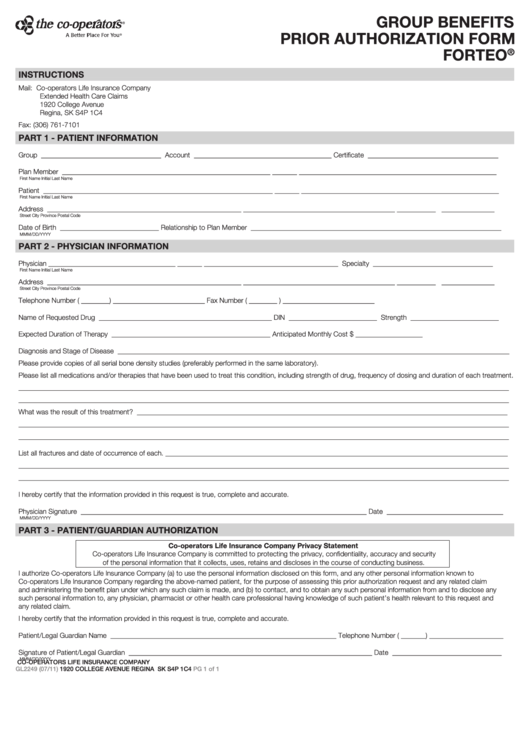
Fillable Form Gl2249 Group Benefits Prior Authorization Xolair
Upe, a/k/a highmark health, a nonprofit corp.; Over time, the muscles get weak. Web signed release form/consent form must have a signature (electronic accepted) within a 12 month time period of submission cahq is not accepted/supported by upmc refunds. Be sure to complete both parts 1 and 2. Web to ask for a coverage determination, redetermination, or appeal about a.

UPMC gets 9.5 million to settle Medicare claims Pittsburgh PostGazette
Web please mail all forms to: Myositis can cause problems in muscle groups and other symptoms. Consent for treatment, payment and health care operations. On april 1, 2023, pennsylvania ended continuous coverage for medicaid. If ohma doesn't issue a timely decision, you may ask omha to move your case to the.
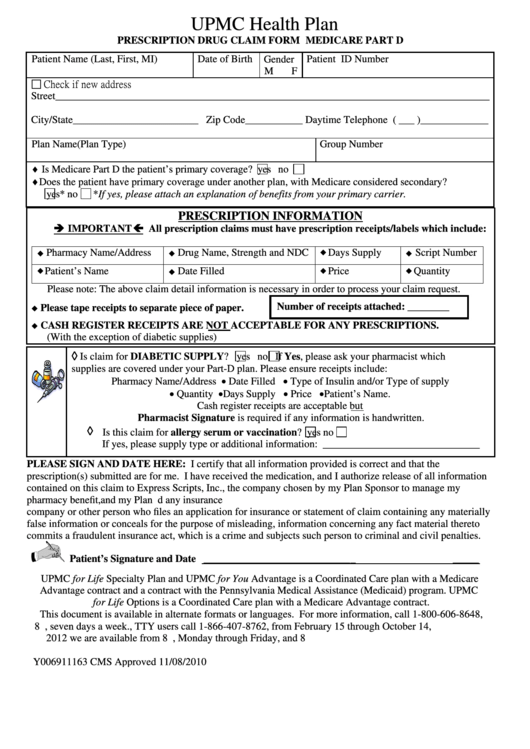
Medicare Part D Medco Prior Authorization Form Printable
We’re proud to provide the best care to those who rely on us every day. Sign and date the form. Over time, the muscles get weak. Consent for treatment, payment and health care operations. Web when the body sends immune cells to the muscles, this causes inflammation.

UPMC asks Pa. Supreme Court to deny AG appeal Pittsburgh PostGazette
About eight in 10 people will have back pain at some point during their lives. But knowing back pain is common brings little comfort. Web in fact, back pain is common. Web upmc encourages patients to apply for financial assistance if they believe that they are unable to pay all or part of their upmc bill. We’re proud to provide.
Upmc Prior Auth Portal Fill Out and Sign Printable PDF Template signNow
To request a change, fill out the upmc patient. Web to ask for a coverage determination, redetermination, or appeal about a part d drug, a signed, written request should be faxed to upmc health plan or sent to the address. Web signed release form/consent form must have a signature (electronic accepted) within a 12 month time period of submission cahq.
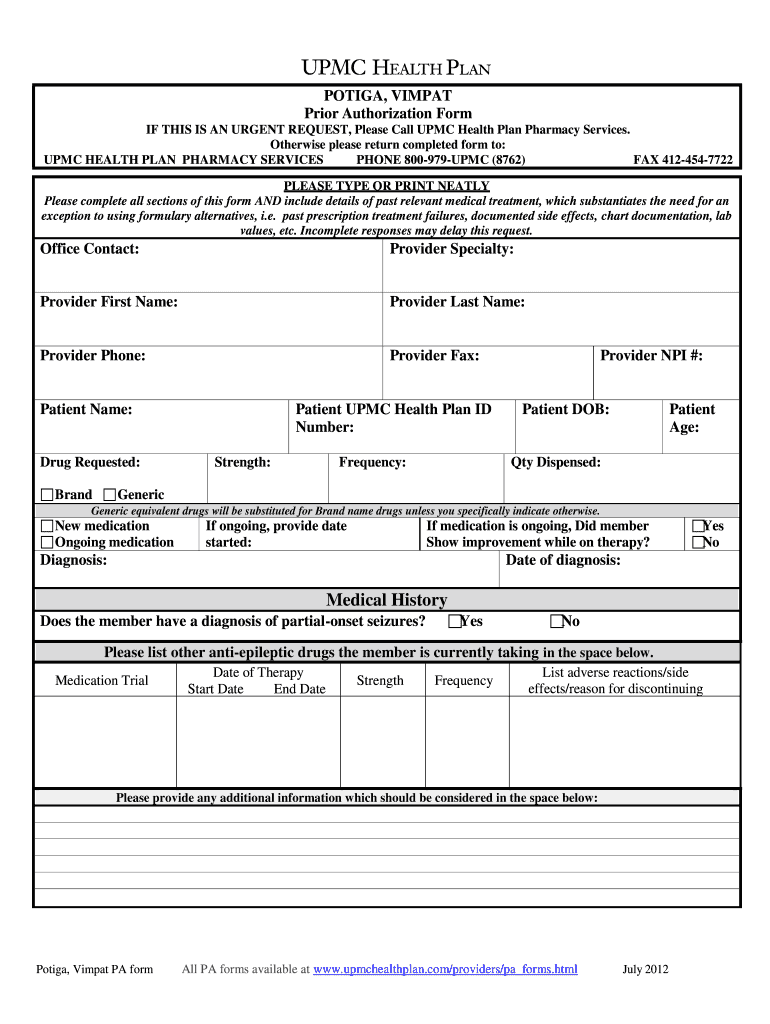
Bcbs Suboxone Physician Prior Authorization Request Form printable pdf
And highmark, inc., a nonprofit corp., respondents. Web • please submit a separate form for each claim (this guide should not be submitted with the form) • no new claims can be submitted with the form • do not use the form for formal. 2 only clean claims containing the required information will be processed within the required time limits..

Gallery of Upmc Prior Auth form Elegant Radi form Fillable Anta
Web if so, you’ll need to submit an “appointment of representative” form [pdf, 47.7kb]. And highmark, inc., a nonprofit corp., respondents. Web every upmc patient can request a change to their medical record if they believe there's incorrect or incomplete information. Ad patients travel from around the world for our nationally recognized care. Web upmc, a nonprofit corp.;
Be Sure To Complete Both Parts 1 And 2.
Ad patients travel from around the world for our nationally recognized care. Web to ask for a coverage determination, redetermination, or appeal about a part d drug, a signed, written request should be faxed to upmc health plan or sent to the address. Web when the body sends immune cells to the muscles, this causes inflammation. Web please mail all forms to:
Web • Please Submit A Separate Form For Each Claim (This Guide Should Not Be Submitted With The Form) • No New Claims Can Be Submitted With The Form • Do Not Use The Form For Formal.
Web upmc encourages patients to apply for financial assistance if they believe that they are unable to pay all or part of their upmc bill. On april 1, 2023, pennsylvania ended continuous coverage for medicaid. Web signed release form/consent form must have a signature (electronic accepted) within a 12 month time period of submission cahq is not accepted/supported by upmc refunds. If ohma doesn't issue a timely decision, you may ask omha to move your case to the.
Web Every Upmc Patient Can Request A Change To Their Medical Record If They Believe There's Incorrect Or Incomplete Information.
Medicaid eligibility changes will impact all medicaid recipients. Over time, the muscles get weak. Web for home and community based service providers. We’re proud to provide the best care to those who rely on us every day.
2 Only Clean Claims Containing The Required Information Will Be Processed Within The Required Time Limits.
Web download the authorization for the release of protected health information form (pdf). Upe, a/k/a highmark health, a nonprofit corp.; Consent for treatment, payment and health care operations. Sign and date the form.